 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
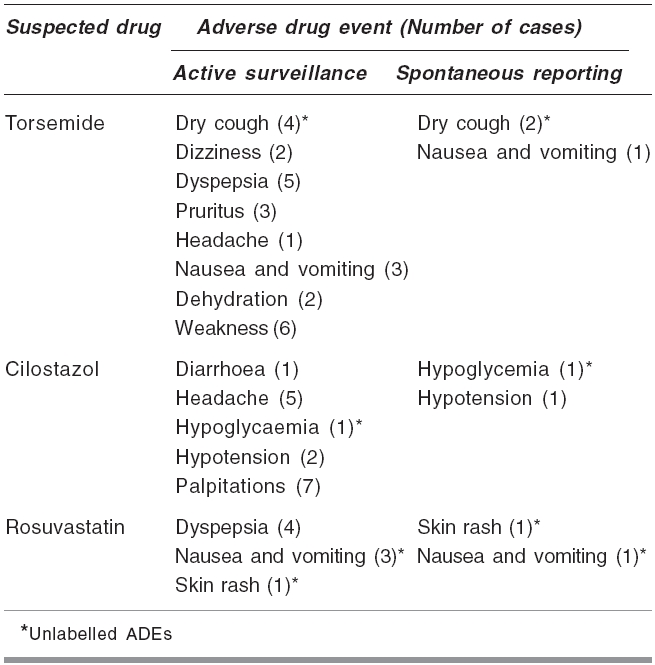
Indian Journal of Pharmacology, Vol. 38, No. 5, September-October, 2006, pp. 363-364 Research Letter Role of active surveillance in improving hospital adverse drug event monitoring Subbanna Prasanna KumarT, Chandy SJ Department of Pharmacology and Clinical Pharmacology, Christian Medical College, Vellore - 632002 Code Number: ph06102 Clinical trials allow only limited assessment of adverse drug events (ADEs) due to their restricted number of patients, short duration and narrow inclusion criteria. About half the drugs which enter the market have serious adverse effects that are detected only after approval.[1] Post marketing surveillance (PMS), through spontaneous reporting (SR) and cohort event monitoring, has an important role in the identification of the side effects which are not seen during pre-marketing trials. It also forms the basis for regulatory and public health decisions. In most hospitals throughout the world, including India, PMS is done through SR. Active monitoring of post-prescription events to newly marketed drugs is not usually done. SR is a well-accepted method, but some of the drawbacks include its selective nature and under reporting. To improve the hospital-based adverse event monitoring, active surveillance of post-prescription events has been suggested.[2] This proposal was followed up by conducting a six month-descriptive study of ADE occurrence and evaluation. This study compared the SR system with the active surveillance system among in-patients in a tertiary care hospital, Christian Medical College (CMC), Vellore, between July and December, 2004. Three newly marketed drugs, i.e. the diuretic, torsemide; the vasodilator, cilostazol; and the antihyperlipidemic, rosuvastatin, were randomly selected for the study. All drugs were approved by the Drugs Controller General of India in 2003 and introduced in our pharmacy from July 2004. In the SR system, ADE reporting cards were kept in each ward. The treating physicians and nurses were requested to enter the cards whenever they suspected ADEs in their patients. The cards were then collected, on a regular basis, and evaluated by pharmacologists associated with the hospital ADE monitoring centre. All spontaneously reported ADEs, associated with study drugs, were selected for the study. In the active surveillance system, all 176 in-patients, consuming any one of the above mentioned drugs, were continuously enrolled from the hospital intranet computer, based on the in-patient prescriptions dispensed by the hospital pharmacy. A pharmacology resident doctor, associated with the hospital ADE monitoring centre, followed up these in-patients on alternate days until their discharge. Physician's notes, nurse's notes and investigational reports attached to the patients' charts were reviewed. To detect incidents not recorded in the medical records, direct patient interviews were conducted by a pharmacology resident, using a structured questionnaire. Questions pertaining to the incidence of similar complaints prior to drug use were included in the questionnaire. Information regarding the patient's age, sex, address, height, body weight, associated illness, use of concomitant drugs was also collected. Naranjo's algorithm score[3] was used to assess the causality of each suspected ADE. Only definite (>9) and probable (5-8) events were taken into consideration. ADEs were classified as serious and non-serious, based on the ICH (International Conference on Harmonization) guidelines.[4] Treating physicians and nurses were kept unaware of the study, to avoid reporting bias, though they were consulted while evaluating the ADEs. Adverse events listed in the summary of product characteristics, enclosed with the drug package at the time of the study, were considered labelled and events not listed were classified as unlabelled. Statistical evaluation was done using two sample tests of proportion. The total number of ADEs, number of labelled and unlabelled ADEs and number of serious and non-serious ADEs, detected through each of the two ADE reporting systems, were used for comparison. P values less than 0.05 were considered significant. A total of 176 patients were followed up, of which 130 (73.9 %) were males and 46 (26.1%) females. A total of 102 (57.9 %) patients were> 60 years, 69 (39.2%) were between 18-59 years and 5 (2.8%) were < 18 years. Forty (76.9%) of the reported 52 ADEs were seen in males and the remaining 12 (23.1%) in females. Forty-three (82.7%) ADEs were seen in patients> 60 years and 9 (17.3%) in patients between 18-59 years. In the SR system, physicians reported 7 ADEs in 7 patients. Through active surveillance, 52 ADEs were identified in 37 of the 176 patients. Twelve of these patients developed more than one adverse event (3 of them had 3 adverse events). A comparison of the ADE detection systems and the description of the ADEs detected during the study is given in [Table - 1] and [Table - 2], respectively. Our study shows that active surveillance is more efficient in detecting adverse events to newly marketed drugs compared to the SR system. As the treating physicians and nursing staff were consulted while evaluating the reported ADEs, the probability of over reporting by the observer (pharmacologist) is minimal. The physicians in our study did not spontaneously report the minor and commonly seen ADEs, but a majority of them were picked up during active surveillance through interviews with patients and nurses' notes. The reasons for such under-reporting and selective reporting might be the lack of manpower and the difficulty in ascertaining the cause of side effects of the drug. Also, many physicians do not see any benefit in investing their time and efforts in reporting minor or common ADEs. Our study also shows that a significant number (15%) of unlabelled ADEs were identified through active surveillance. The labelled ADEs are the extension of the pharmacological activities of the drugs usually identified during initial trial studies, whereas the unlabelled events are usually idiosyncratic in nature and depend on variables such as age, sex, associated illness and so on. In addition to spontaneously reported serious ADEs, many minor, labelled and unlabelled ADEs could be identified, by actively monitoring the post prescription events. This becomes crucial when monitoring newly marketed drugs. Our objective was to compare the efficiency of active monitoring over SR in detecting the incidence of ADEs associated with newer drugs. Hence, the control groups receiving standard old drugs were not included in the study. Similarly, compounding factors such as drug interactions, coexisting diseases, severity of the disease and status of the organs influencing drug pharmacokinetics, which can influence the occurrence of ADE, were not considered as the study population was the same for both the reporting systems. The limitations of our study are the small number of drugs and subjects selected for monitoring, short duration and, thereby, the inability to pick up long-term toxicities. The major constraint with the active surveillance system is the allocation of manpower. In the present study, a pharmacologist and a pharmacology resident doctor spent about one hour per day for 6 months. The services of pharmacologists and nurses, who contributed significantly to our study, could be utilised for hospital ADE monitoring. Hence, we suggest that hospital ADE monitoring centres institute active surveillance systems to suit their bed strength and resources available for ADE monitoring. The deluge of new drugs in the Indian market demands a focus on their adverse effects. Novel drugs, wherein minimum human pharmacology data is available, and drugs with a narrow therapeutic index and zero order kinetics, should be given importance over other drugs in case of limited resources. In conclusion, we suggest supplementing SR-based hospital ADE monitoring systems with an active surveillance system to monitor the safety profile of newly marketed drugs at all tertiary care hospitals. This will help in providing better patient care as well as offer substantial data support to the recently initiated National Pharmacovigilance Programme in India. Acknowledgments The authors deeply appreciate the co-operation extended by the physicians, nursing staff, pharmacy and medical records personnel of the Christian Medical College, Vellore.References
Copyright 2006 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph06102t2.jpg] [ph06102t1.jpg] |
| |||||||||

{kind=link}
{kind=link}