 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
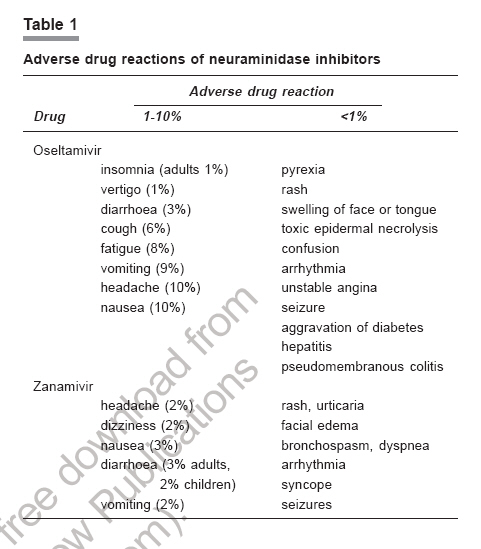
Indian Journal of Pharmacology, Vol. 38, No. 6, November-December, 2006, pp. 383-389 Educational Forum Frontline defense against the next pandemic: Antivirals for avian flu Khan SohilA, Rao PadmaG M, Kumar P, Rodrigues G Department of Pharmacy Practice, Manipal College of Pharmaceutical Sciences, Manipal-576 104 Date of Submission: 13-Mar-2006 Code Number: ph06112 Abstract A pandemic of the human influenza virus has caused extensive morbidity and mortality around the world. The mechanisms involved in the emergence of new influenza viral strains and the epidemiological factors leading to pandemics are unpredictable. The spread of the virus and the challenges encountered in its management are discussed, along with a review on the antivirals against avian influenza. Till date, neuraminidase inhibitors remain the mainstay of management as they are well tolerated and less likely to promote the development of drug resistance, compared to the conventional adamantanes. Details on the clinical effects of antivirals on the infection, safety profile, status in clinical practice and drug resistance are covered in this paper. Future prospects and research to fight the pandemic are also addressed. An outbreak of this infection in various Asian countries emphasises the need for a collaborative approach from healthcare experts, governments and media, to control and curb the spread of infection worldwide.Keywords: Antiviral drugs, bird flu, drug resistance Introduction An influenza pandemic has always been a global threat.[1] Flu pandemics occur in cycles, with the last three occurring in 1918, 1957 and 1968.[2] Like a pandemic, the avian influenza scare came in waves. In 1997, the first case of the H5N1 strain of bird flu emerged in Hong Kong, infecting 18 people and killing 6.[3],[4],[5],[6] In late 2003, it struck again, affecting more than 120 people, and at least 60 deaths were reported over the next two years.[7] Recent analysis showed that the pandemic of 1918 and 1919 killed 50-100 million people.[1] Today, with a world population which is more than three times than that of 1918, even a relatively mild pandemic could kill many millions. No one knows when the next outbreak will be, but it is due any time from now! Most important, it is difficult to know what structure the avian flu virus will take. The virus can improve its transmissibility among humans via two principal mechanisms. The first is a "reassortment" event in which genetic material is exchanged between human and avian virus during co-infection of a human and a pig. The second mechanism is a more gradual process of adaptive mutation, whereby the capability of the virus to bind to human cells increases during subsequent infections of humans.[8] Currently H5N1, is the virus strain of avian influenza in circulation in Asia.[9],[10] From mid December 2003 through early February 2004, poultry outbreaks caused by the H5N1 virus were reported in 8 Asian countries, which include the Republics of Korea and Indonesia, Vietnam, Japan, Thailand, Cambodia, Republic of Indonesia and China and Lao People's Democratic Republic.[8] Are we prepared to defend ourselves against the next pandemic? The key step is to rapidly ramp up research related to the production of an effective vaccine against the virus. Vaccine development is rather slow. Even if the subtype of the pandemic strain is isolated, manufacturing a vaccine will take around 6-8 months. The 1918 Spanish influenza virus killed 25 million people worldwide, in 25 weeks[11],[12],[13] and hence a 6-8 months' period may prove too long a wait. Given the capacity of all the current international vaccine manufacturers, supplies during the 6-8 months' period would be limited to fewer than a billion monovalent doses. Hence, as many health officials agree, antivirals are likely to be the first line of defense. Role of antivirals The use of antivirals is recommended for the control of seasonal and pandemic influenza. Four drugs are currently available for the treatment and/ or prophylaxis of influenza infections: (1) Adamantanes (amantadine and rimantadine) (2) Neuraminidase (NA) inhibitors (zanamivir and oseltamivir). Adamantanes are effective only against influenza A and are associated with a rapid emergence of drug resistance and several toxic effects. Adamantine-resistant influenza A isolates are genetically stable; can be transmitted to susceptible contacts; are pathogenic and can be shed for prolonged periods in immunocompromised patients taking the drug. This limits the use of the adamantanes for the treatment of influenza. A meta analysis,[14] on the role of antivirals against influenza, has concluded that the use of amantidine and rimantidine should be discouraged. NA inhibitors (oseltamivir and zanamivir) should only be used in a serious epidemic or pandemic along with other public health measures. As concerns over an outbreak mounted, governments around the world competed to stockpile Tamiflu (a Roche-licensed product of oseltamivir) as the treatment option against influenza. Oseltamivir was discovered in the mid '90s, shortly after scientists in Australia-based Biota learned that the neuraminidase protein of the flu virus could be inhibited.[15] A second type of antiviral available in the market is zanamavir (a GlaxoSmithKline product marketed as Relenza). Primarily, when it was first launched during the 2000-01 flu season, the drug was a dud because it was packaged as an inhaled powder. But faced with a virus as deadly as H5N1, it became the mainstay of management in avian flu influenza. As a class, NA inhibitors are effective against all neuraminidase subtypes and, therefore, against all strains of influenza, which is important considering the epidemic and pandemic threat. Adamantanes are effective only against sensitive strains of influenza A. Hence, NA inhibitors, if used rationally, have a greater potential for combating the influenza infection.Clinical review of oseltamivir Oseltamivir was the first orally active NA inhibitor. With increasing fears regarding the potential of a new influenza pandemic, oseltamivir has received substantial media attention. As the production capacity is limited, governments are stockpiling the drug. Mechanism of action Oseltamivir, a prodrug, is hydrolyzed to the active drug, oseltamivir carboxylate. It inhibits the NA of influenza virus with the possibility of alteration of virus particle aggregation and release. In clinical studies of influenza virus, 1.3% of post-treatment isolates had decreased the NA susceptibility to oseltamivir carboxylate. The enzyme (sialidase, expressed on the NA viral surface) hydrolyzes terminal sialic acid residues from glycoproteins, oligosaccharides and glycolipids and is required for infectivity of the virus; the NA may be essential for elution of newly synthesised virions from infected cells.[16], [17] Activity against avian influenza In vitro and in vivo (mice) studies have demonstrated that oseltamivir inhibited avian influenza (H5N1 and H9N2) and viral replication, and prevented death in mice. It also inhibited the replication of human isolates of influenza A (A/HK/156/97 [H5N1] and A/HK/1074/99 [H9N2]); the EC 50 (concentration required to inhibit viral replication by 50%) values of oseltamivir were 7.5 and 12 micromolar, respectively. Oseltamivir also inhibited the activity of viral NA in vitro; the IC 50 (mean concentration of oseltamivir required to inhibit NA activity by 50%) was 7 ± 0.9 nanomolar for A/HK/156/97 and 15 ± 0.7 nanomolar for A/HK/1074/99. Mice, infected with H5N1 or H9N2 viruses and treated with oseltamivir, were completely protected from death (the lowest effective dose was 1 mg/kg/day); had significantly reduced virus load in the lungs ( P < 0.01); and had undetectable level of virus in the brain ( P < 0.05 for mice treated with 0.1 mg/kg/day).[18] Oseltamivir failed to prevent death or extend the length of survival in mice when treatment was delayed by 60 or more hours after inoculation. The combination of oseltamivir and rimantadine significantly increased the number of survivors and the length of survival in mice inoculated with high doses of virus as compared with mice treated with the same doses of oseltamivir and rimantadine, administered individually.[18] Oseltamivir inhibited virus replication in a series of tissue cultures, representing each of the 9 NA subtypes. The EC 50 of oseltamivir required to inhibit virus replication ranged from 1 to 42 micromolar. The IC 50 required to reduce virus NA activity in each of the NA subtypes ranged from 1.9 to 69.2 nanomolar, indicating that oseltamivir inhibited NA activity. Mice, infected with H5N1 or H9N2 viruses and treated with oseltamivir, were completely protected from death (at 0.1 and 1 mg/kg/day, respectively); had significantly reduced virus titers in the lungs (at 1 mg/kg/day); and had undetectable levels of virus infectivity in the brain (at 0.1 and 1 mg/kg/day respectively).[19] In a test of oseltamivir efficacy, 90% and 65% of mice survived when treatment was delayed by 24 and 60 h, respectively, after inoculation with H5N1. The sensitivity to oseltamivir was similar in viruses obtained from murine lungs, following treatment and in the original virus used for inoculation, indicating that resistance did not develop in oseltamivir-treated mice.[19] An avian influenza virus H7N7, which caused an outbreak of avian influenza in poultry farm workers in the Netherlands in 2003, was also susceptible to oseltamivir. The IC 50 of oseltamivir for the H7N7 virus was 1.29 nanomolar (95% CI 1.19 to 1.40 nmol/L), which is within the range of IC 50 for zanamivir-sensitive H1N1 and H3N2 clinical isolates (0.2 to 6.8 nmol/L, dependent on isolate and assay).[7] Pharmacokinetics Oseltamivir is well absorbed orally and the concentration for NA inhibition is 0.003 mcg/mL or greater.[16] The mean maximum concentrations for oseltamivir phosphate and oseltamivir carboxylate, after a multiple 75 mg twice daily oral dose, were 65.2 and 348 ng/mL, respectively. The area under the curve (AUC) is 112 and 2719 ng.h/mL, respectively.[20] Oral oseltamivir phosphate is readily absorbed and extensively converted to the active form, oseltamivir carboxylate, predominantly by hepatic esterases. The drug is 3-42% protein bound and the volume of distribution is 23-26 litres.[20] The metabolite is eliminated entirely (greater than 99%) by renal excretion. The elimination half-life of oseltamivir phosphate (prodrug) is 1-3 h and its metabolite oseltamivir carboxylate (active drug) is 6-10 h.[16],[21] Indications The treatment and prophylaxis of avian influenza,[22] of uncomplicated acute illness should be initiated in adults and children (above 1 year), who have been symptomatic for no more than 2 days. This applies for prophylaxis of influenza and hemopoietic stem cell transplant. Safety profile Oseltamivir has few adverse effects when administered for either treatment or prophylaxis. Adverse drug reactions are mentioned in [Table - 1].[23],[24],[25] Place in clinical practice Although oseltamivir has shown efficacy in the treatment of influenza, these findings must be placed in a clinical perspective. The agent has reduced the duration of symptoms by approximately 1 day, a benefit which may not be worth the effort to many patients with moderate illness, considering the need to gain rapid access to a physician and a prescription, and to begin treatment within 24 h, for maximum benefit. The cost of treatment with these agents will be substantially higher as compared to the routine prevention with vaccine. A method of rapid viral diagnosis is not readily available as yet and hence many patients will be misdiagnosed and treated inappropriately. With regard to prophylaxis, influenza vaccine is preferred to the more costly therapy with oseltamivir. Comparative studies between drugs and vaccine are lacking. At present, the prevention of influenza with the current-season vaccine is preferred and is less expensive than treatment or drug prophylaxis. Oseltamivir should be considered as an alternative for treatment of infection, primarily in high-risk groups (elderly patients, underlying cardiovascular/ respiratory disease, renal dysfunction). The routine use of these agents in young patients is questionable. The selection of one agent over the other (oseltamivir vs zanamivir) will likely to be determined by patient preference (inhalation Vs tablet) and comparative cost. A direct comparison of zanamivir with oseltamivir is needed with respect to safety, efficacy and patient compliance.[26] Clinical review of zanamivir It is an inhalational antiviral agent against influenza. It was discovered in 1989 at the Australian Biotechnology Company, Biota Holdings, working in conjunction with the Commonwealth Scientific and Industrial Research Organisation (CSIRO) and Victorian College of Pharmacy. Mechanism of action Zanamivir inhibits the NA of influenza virus, altering virus particle aggregation and release. It is a selective inhibitor of influenza A and B virus NA and inhibits viral cleavage of sialic acid from cell surface glycoconjugates, which inhibits the release of newly formed virus from the surface of infected cells. It also prevents viral spread across the mucous lining of the respiratory tract.[27] Activity against avian influenza An avian influenza A virus (H7N7), which caused an outbreak in commercial poultry farms in the Netherlands in 2003, was found to be susceptible to zanamivir in vitro. The IC 50 was 3.94 nmol/L (95% CI 3.61 to 4.29 nmol/L), which is within the range of IC 50 for zanamivir-sensitive H1N1 and H3N2 clinical isolates (0.3 to 13.1 nmol/L).[7] Zanamivir inhibited in vitro replication and NA activity of 3 strains of avian influenza A (H5N1, H9N2, and H6N1); provided complete protection from death in mice infected with strains of H5N1, H9N2, and H6N1, when administered intranasally at doses of 50 mg/kg twice daily; and significantly reduced virus titer in murine lungs. In vitro EC 50 of zanamivir, to effectively inhibit virus replication, ranged from 8.5 to 14 micromolar. Zanamivir also inhibited the activity of viral NA in vitro . The IC 50 of zanamivir required to reduce NA activity ranged from 5 to 10 nanomolar. Although virus titers in murine lungs were significantly reduced for each of the viruses tested, the only strain reduced to undetectable levels was H9N2.[28] It was tested for inhibition of replication and NA activity in tissue cultures of a series of avian influenza A viruses, representing all 9 NA subtypes, and the EC 50 to inhibit virus replication ranged from 4 to 58.3 micromolar. The IC 50 required to reduce virus NA activity ranged from 2.2 to 30.1 nanomolar, indicating that zanamivir inhibited NA activity.[19] Pharmacokinetics Zanamivir is marketed as a dry powder for inhalation as it is not orally bioavailable. Peak response against influenza A/B via inhalation is 72 h.[25] The time to peak concentration via inhalation is 0.75 to 2 h. Bioavailability via oral route is 2%, whereas by inhalation it is 4% to 25%. Zanamivir concentrations in the sputum were found to be least 52 fold above the IC 50 , 6, 12 and 24 h after a single 10 mg inhaled dose of zanamivir.[29],[30],[31] The median zanamivir concentrations in the sputum were 1336, 304 and 47 ng/mL at 6, 12 and 24 h after a single 10 mg inhaled dose in healthy volunteers (n=6).[30] Systemic administration showed high blood concentrations, but essentially no antiviral activity and was related to poor respiratory secretion penetration (supports cell surface activity). The volume of distribution was 16 L with minimal to no metabolism. Renal excretion was 4-17% (intranasal) and 87% (intravenous) and the elimination half life 1.6 -5.1 h.[29],[30],[31] Indications The treatment of uncomplicated acute illness due to influenza virus in adults and children, older than 7 years, should only be initiated if symptomatic for no more than 2 days. It is FDA approved against influenza treatment and prophylaxis. It is also used against avian influenza, influenza virus A/B.[32],[33],[34] Safety profile In general, zanamivir is well tolerated. Studies till date, suggest that the adverse effects are primarily minor transient upper respiratory and gastrointestinal symptoms.[35],[36],[37] [Table - 1] Place in clinical practice The drawbacks with zanamivir are as follows.
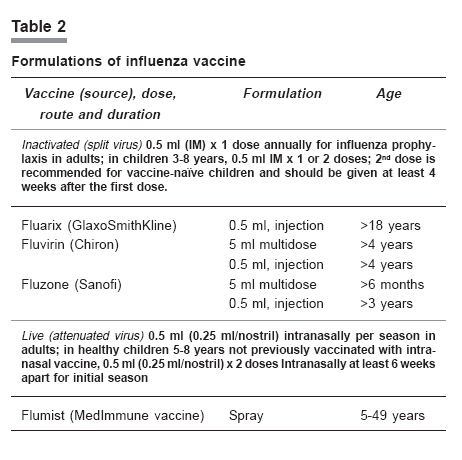
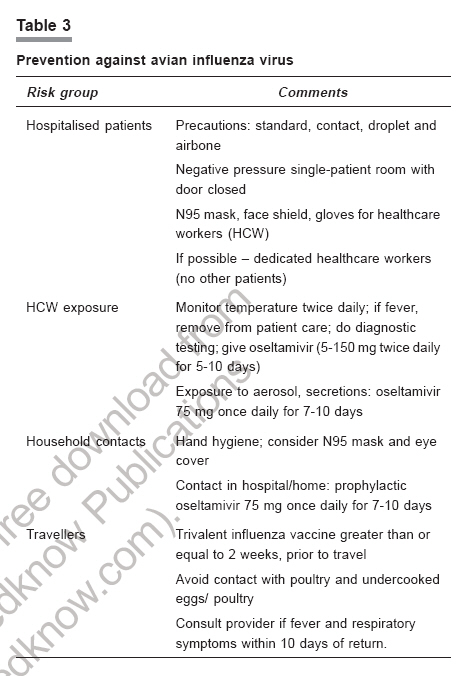
Prophylaxis of influenza with antiviral agents, including zanamivir, is not a substitute for the influenza vaccine and should only be used as an adjunct to the vaccine.[26] When a 28-day regimen of inhaled zanamivir, 10 mg daily, was initiated on the same day as administration of the 1997-1998 trivalent influenza vaccine, antibody production was not affected in a placebo-controlled trial of healthy volunteers (n=138). The hemagglutination inhibition titers 4 weeks after influenza immunisation were statistically similar in the zanamivir and placebo groups. This data suggest that concomitant zanamivir does not compromise the immune response to the influenza vaccine. Further studies in high-risk groups are required.[38] Cost effectiveness Zanamivir, if used within 36 h of symptom onset, can reduce the health-care cost in high risk groups (patients who are 65 years and older) with influenza. A cost-effective study used efficacy data from an Australian clinical trial to model an estimation of healthcare cost in the high risk population. Cost savings are based on avoidance of hospitalisations.[39] Again future studies are needed to demonstrate the reduction of hospitalisation rate with zanamivir in the high-risk group. Resistance against antivirals A key advantage of the NA inhibitors and a major difference from the adamantanes is that the development of resistance is very rare. But emergence of resistance against the NA inhibitors is a matter of immediate concern that is disabling our influenza defenses. Two studies in Japan confirmed the oseltamivir resistant cases.[40],[41] However, the high rate of emerging resistance in these studies may have been due to the use of insufficient doses of the drug and the resultant failure to eradicate the virus. No virus resistant to zanamivir has yet been isolated from immunocompetent patients after treatment. Zanamivir resistance developed in an immunocompromised infant infected with influenza B virus.[42] Structural analysis[43] predicted that the chemical structure of oseltamivir, differing from zanamivir, could facilitate the development, survival and propagation of drug-resistance virus. Molecular analysis[44] showed that the amino acid E276 must rotate and bond with R224 to form a pocket for the side chain of oseltamivir. The mutations of R292K, N294S and H274Y inhibit this rotation and prevent the pocket formation, resulting in oseltamivir resistance. The mutations allow the binding of natural sialic acid substrate, so that the mutated virus can survive and propagate. In contrast, the binding of zanamivir does not require any reorientation of amino acids, so these mutated viruses remain sensitive to that drug. It is worrisome that personal stockpiling of oseltamivir is likely to lead to the use of insufficient doses or inadequate courses of therapy which can promote resistance. This may lessen the usefulness of first line pharmacotherapy defense against influenza.Future therapy and research Combating a disease as nimble and adaptive as influenza requires scientists and healthcare professionals to look for new products and alternative methods of production apart from the available antivirals. Current influenza virus vaccines consist of 3 components: (a) an H1N1 hemagglutinin [HA] subtype 1 (b) a neuraminidase [NA] subtype 1 (c) an H3N2 influenza A virus and an influenza B virus. Specifically the 2005-2006 vaccine formulation is made up of the A/New Caledonia/20/99 (H1N1), A/California/7/2004 (H3N2), and B/Shanghai/361/2002 viruses.[45] Vaccine efficacy for the inactivated vaccine in preventing influenza is about 80%. However, it varies by year depending on the match between the vaccine strains and the epidemic strain. Protection begins about 2 weeks after vaccination and generally persists for 6 months (only about 4 months in the elderly). Protection with live vaccine appears to be similar and probably superior for new variants of influenza A H1N1 and for influenza B. Live attenuated intranasal vaccine is generally well tolerated, but there may be mild symptoms of an upper respiratory infection. Both live and inactivated vaccines are grown in eggs. So, egg hypersensitivity represents a contraindication to either.[46] The available influenza vaccine formulation is depicted in [Table - 2].[47] The measures to prevent the spread of influenza A (H5N1) are provided in [Table - 3].[47] Constant research is ongoing in the area of vacci- nation.[48],[49],[50],[51] The issues to be considered in developing new and better vaccines are price per dose, speed and ease of production, choice of substrate to grow the virus in or to express viral antigens, cross-protection for variant strains, efficacy in general and in immunologically naive populations, safety and acceptance by the regulatory agencies and the public. Some of the ways in which scientists have ventured beyond the conventional in constructing a bird flu defense are:
Conclusion It is not clear whether H5N1 avian influenza virus threatens an imminent pandemic. Most indications, however, suggest that it is just a matter of time: witness the increasing number of H5N1 infections in humans and animals, the ongoing genetic changes in the H5N1 Z genotype with increased pathogenecity, and the existence of this virus in Asia. The older class of antiviral drugs, the M2 inhibitors amantidine and rimantidine, could potentially be used against pandemic influenza, but resistance to these drugs can develop rapidly. Oseltamivir and zanamivir can reduce the severity and duration of illness caused by seasonal influenza. Antiviral resistance to NA inhibitors has been clinically negligible so far, but is likely to be detected during the widespread use during a pandemic. A rational use of antivirals with a better understanding of the pharmacology and clinical research is needed for an effective defense. The need of the hour is to accelerate the clinical research related to the production of effective vaccines and pharmacotherapy along with the established measures to prevent and treat this pandemic. Despite the efficacy of both killed and live influenza virus vaccines, there is room for new developments. Simultaneously, basic research on the ecology and biology of influenza viruses, studies on the epidemiologic role of various animal and bird species, and work on early interventions and risk assessment are to be carried out.References
Copyright 2006 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph06112t1.jpg] [ph06112t2.jpg] [ph06112t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}