 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Pharmacology, Vol. 38, No. 6, November-December, 2006, pp. 390-396 Educational Forum Monoclonal antibodies: Targeted therapy Gupta N, Srivastava A Intas Biotechnology/Oncology, Plot No. 423/P/A/GIDC, Sarkhej Bavla Highway, Moraiya, Tal: Sanand, Ahmedabad-382 210 Date of Submission: 02-Feb-2006 Code Number: ph06113 Abstract In an ongoing quest to improve the therapeutic arsenal against cancer, a fourth weapon other than surgery, chemotherapy and radiotherapy has emerged, i.e. targeted therapy. Targeted therapy includes, tyrosine kinase receptor inhibitors (small molecule inhibitors like imatinib, gefitinib, erlotinib), angiogenesis inhibitors (bevacizumab), proteasome inhibitors (bortezomib), biological response modifiers (denileukin diftitox) and monoclonal antibodies (MAbs). The remarkable specificity of MAbs as targeted therapy makes them promising agents for human therapy. Not only can MAbs be used therapeutically to protect against disease, they can also be used to diagnose a variety of illnesses, measure serum protein and drug levels, type tissue and blood and identify infectious agents and specific cells involved in immune response. About a quarter of all biotech drugs in development are MAbs, and about 30 products are in use or being investigated. As a majority of the MAbs are used for the treatment of various hematological and nonhematological malignancies, their role in cancer is discussed.Keywords: Antibodies, chemotherapy, immunity, malignancy. Introduction 'Targeted therapy' is a general term that refers to a medication or drug that targets a specific pathway by attacking or blocking important targets. The targets themselves are typically various molecules (or small particles) in the body that are known or suspected to play a role in various diseases. One long-held dream is that the specificity of immune mechanisms could be harnessed against tumor cells. Monoclonal antibodies (MAbs) are so called because they arise from a single cell type. They act by recognizing the protein on the surface of the cell and then lock onto it. They are produced in the laboratory from a single clone and recognize only one antigen. MAbs are typically made by fusing a normally short-lived antibody producing β-cell to a rapidly dividing cell, such as cancer cell (often referred to as 'immortal cell'). The resulting hybrid cell, or hybridoma, multiplies rapidly; creating a clone that produces large quantity of the antibodies. In 1975, Kohler and Milstein first fused lymphocytes to produce a cell line, which was both immortal and a producer of specific antibodies. The two scientists were awarded the Nobel Prize for Medicine in 1984 for the development of this 'hybridoma.' The value of hybridomas to the field was not truly appreciated until about 1987, when MAbs were regularly produced in rodents for diagnostics. Targeted therapies Several classes of compounds included in targeted therapy are as follows:
MAbs of different origin
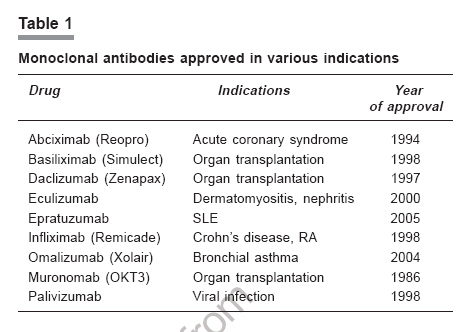
Recombinant engineered MAbs Various approaches to overcome the problem of immunogenicity have been tried. One approach is to take the DNA that encodes the binding portion of monoclonal mouse antibodies and merge it with human antibody-producing DNA. A mammalian cell culture is used to express DNA that produces these half-mouse and half-human antibodies (bacteria cannot be used for this purpose, since they cannot produce this kind of glycoprotein). Depending on the size of the part of the mouse antibody used, it could be chimeric antibodies or humanized antibodies. Another approach involves genetically engineered mice that produce more human-like antibodies. Engineered MAbs have the advantages of decreased immunogenicity, enhanced half-life and optimized specificity. Some of the MAbs approved for various indications (except cancers) are shown in [Table - 1]. MAbs in cancer One possible treatment for cancer involves MAbs that bind only to cancer cell-specific antigen which induce an immunological response in the target (cancer) cell. Such MAbs could also be modified to deliver toxins, radioisotopes, cytokines or other active conjugates. It is also possible to design bispecific antibodies that can bind through their Fab regions to both the target antigen and to a conjugate or effecter cell. In fact, every intact antibody can bind to cell receptors or other proteins with its Fc region. Most of the therapeutic antibodies act differently in cancer:
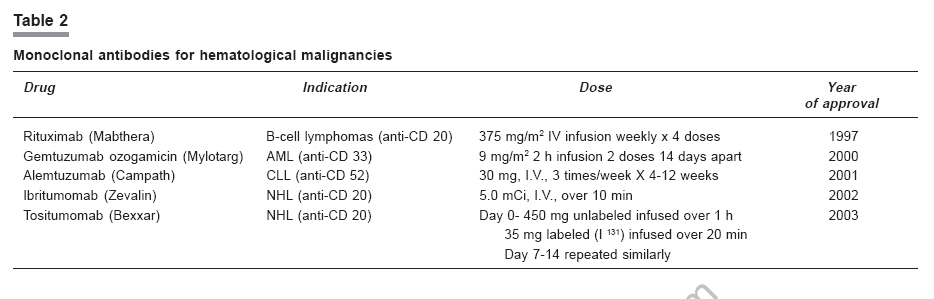
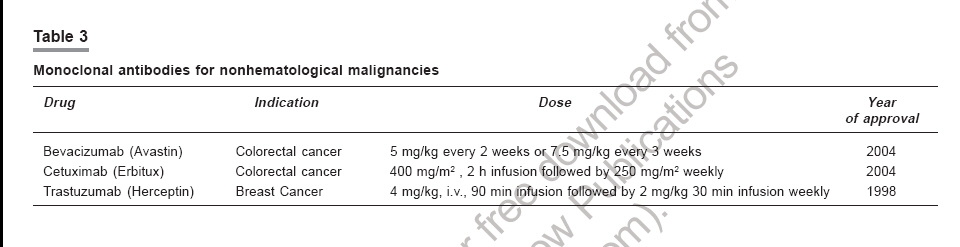
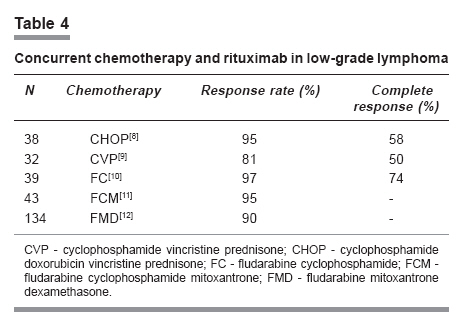
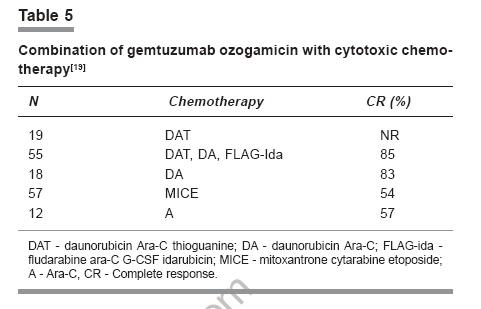
MAbs for hematological malignancies The treatment of hematological malignancies has been largely based on chemotherapy and radiotherapy. Although improvement in response and survival rates has been seen over the years, poor response or relapses occur in a significant proportion of patients. Moreover, conventional cytotoxic therapy is often associated with significant morbidity. Monoclonal antibodies have emerged as important therapeutic agents in a number of hematological malignancies.[1],[2] The main advantage of MAbs therapy compared to conventional chemotherapy is that the former specifically targets surface antigens that are uniquely expressed on tumor cells. Since the introduction of rituximab as the first targeted MAb therapy for β-cell lymphoma relapse in December 1997, MAbs are extensively used in β-cell lymphoproliferative disorders.[3],[4] The application of MAbs, particularly directed at the CD33 and CD45 antigens, has been explored in acute myeloid leukemia with naked, radioimmune or antibody-chemotherapy conjugates. The radioimmunotherapy for non-Hodgkins lymphoma (NHL), using two anti CD20 antibodies with different radioisotopes, have been approved for clinical use. The antibodies for hematological malignancies directed at antigen targets including but not limited to CD30, CD5, CD80 and CD23 are at various stages of development. Indeed, some clinical activity has been observed with CD30, CD80 and CD23 antibodies in Hodgkin's disease, low grade NHL, and chronic lymphatic leukemia (CLL ) , respectively.[5] Rituximab (anti CD20) and alemtuzumab (anti CD52) have proven efficacy in different clinical trials for the treatment of NHL[3] and CLL, respectively. Rituximab Rituximab is a chimeric humanized MAb that binds with CD20 molecule found on most β-cells and is used to treat β-cell NHL. Rituximab has proven efficacy against a wide range of β-cell malignancies, including follicular lymphoma, small lymphocytic lymphoma, marginal zone lymphoma, Waldenstrom's macroglobulinemia, mantle cell lymphoma, diffuse large-cell lymphoma and post-transplant lymphoproliferative disorders.[3],[4],[6] The mechanism of action of rituximab is ADCC, CDC and apoptosis Rituximab as single agent: In indolent lymphoma that has progressed after prior chemotherapy, rituximab as a single agent is associated with 50-60% response rates in the relapsed setting and 60%- 75% as front-line therapy. Rituximab in combination chemotherapy : Rituximab in vitro enhanced sensitivity to chemotherapy, thus creating a rationale for combined modality treatment.[7] The greatest synergy or additive effects were seen with the anthracycline, doxorubicin. Combination chemotherapy regimens with rituximab have been used in patients with low-grade lymphomas, like CHOP[8] CVP,[9] FC,[10] FCM[11] and FMD[12]. [Table - 4] The R-CHOP regimen was associated with a response rate of 95%, including 58% complete responders. In a recent study, 428 patients with untreated advanced-stage follicular lymphoma were randomly assigned for treatment with CHOP alone (n=205) or combined with rituximab (R-CHOP; n=223). Treatment with R-CHOP reduced the relative risk for treatment failure by 60% and significantly prolonged the time to treatment failure. Treatment with R-CHOP resulted in a significantly higher overall response rate of 96% compared to 90% for CHOP.[13] In a European trial, FCM plus rituximab was compared to FCM alone in previously untreated follicular lymphoma or mantle cell lymphoma. In the 43 subset patients with follicular lymphoma, combination therapy was associated with a response rate of 95% versus 68% for FCM alone and a higher complete response rate as well 36% Vs. 15%. A rituximab combined CVP regimen in previously untreated low-grade lymphoma has shown a response rate of 81%, with 50% complete response. Rituximab has been added as part of sequential therapy after chemotherapy, or as a consolidation treatment in patients who have already responded to chemotherapy. Rituximab was also used with biological-response modifiers in patients with relapsed low-grade lymphoma. These include interferon alfa, IL-2, IL-12 and GM-CSF. Alemtuzumab Alemtuzumab is a humanized antibody that reacts with the CD52 molecule that is found on both normal and malignant B- and T-lymphocytes, as well as NK-cells, monocytes, macrophages and tissues of the male reproductive system.[14] It was approved in May 2001 based on objective responses in patients with CLL that had relapsed after treatment with fludarabine. Alemtuzumab was also evaluated in 50 patients with previously treated indolent lymphoma. Alemtuzumab, when given with rituximab, has produced a response in 10 out of 22 patients with CLL and it would be rational to use this combination in low-grade lymphomas.[15] Alemtuzumab is the foundation of many eradication-based treatment approaches because of its ability to achieve clinical remissions and to successfully purge minimal residual disease (MRD) from both blood and bone marrow in B-CLL patients. The ability to clear MRD from bone marrow in patients achieving clinical complete response (CR) using alemtuzumab is a significant step forward in the treatment of B-CLL, and supports treatment strategies combining alemtuzumab with other agents. Purging of MRD from both blood and bone marrow also enables patients for autologous hematopoietic stem cell transplantation, a strategy to achieve long-term remission.[16] Forty-one consecutive CLL patients underwent allogeneic hematopoietic cell transplantation after conditioning with fludarabine, melphalan and alemtuzumab. The alemtuzumab-based regimen was feasible and effective in patients with CLL with a relatively low rate of graft versus host disease . However, transplant related mortality remains relatively high as a result of a variety of viral and fungal infections. Studies are on to test the efficacy of reduced doses of alemtuzumab in this group of highly immunosuppressed patients.[17] Gemtuzumab ozogamicin Gemtuzumab ozogamicin is a humanized MAb directed against CD33 linked to a calicheamicin derivative. This molecule is a member of the enediyne family of antitumor antibiotics, which are more cytotoxic than other clinically used anticancer agents. Gemtuzumab ozogamicin is rapidly internalized after binding to its target, followed by the release of the potent antitumor calicheamicin derivative. This compound-induced double-stranded DNA breaks, resulting in apoptosis. It has been observed that within 3 to 6 h of infusion, a near-complete saturation of CD33 antigenic sites is reached for AML blasts, monocytes and granulocytes.[18] It is approved for the treatment of elderly patients (≥ 60 years) with CD33+ AML in first relapse and who are not considered candidates for cytotoxic chemotherapy. Gemtuzumab ozogamicin as a single agent clearly serves a role in the setting of relapsed AML. Several groups are evaluating targeted therapy in combination with cytotoxic chemotherapy as a frontline therapy.[19] [Table - 5] Gemtuzumab has been used in combination with all-trans retinoic acid (ATRA) in the treatment of acute promyelocytic leukemia (APML) with favorable response.[20] Radiolabeled anti-CD20 antibodies Radiolabeled antibodies such as yttrium 90-ibritumomab tiuxetian (Y 90), indium 111-ibritumomab (In 111) and iodine 131-tositumomab (I 131sub ) may be even more efficacious than MAbs in the treatment of NHL. In relapsed indolent lymphoma, response rates of up to 80% have been noted with ibritumomab tiuxetian (Y90), compared to 56% with rituximab.[21] Tositumomab and iIodine (I 131) tositumomab is administered in two steps. The dosimetric step determines individual patient pharmacokinetics, allowing a patient- specific dose to be calculated. This is followed by the therapeutic step, with administration of the therapeutic dose between 7 and 14 days after the dosimetric dose.[22] Advanced-stage follicular β-cell lymphoma is considered incurable. Anti CD20 radioimmunotherapy is effective in patients who have had a relapse after chemotherapy or who have refractory follicular lymphoma, but it has not been tested in previously untreated patients. Seventy-six patients with stage III or IV follicular lymphoma received a single course of 131I-tositumomab as initial therapy.[23] This consisted of a dosimetric dose of tositumomab and 131I-labeled tositumomab followed one week later by a therapeutic dose, delivering 75 cGy of radiation to the total body. Ninety-five percent of the patients had overall response, and 75 percent had a complete response. The use of polymerase chain reaction (PCR) to detect rearrangement of the BCL2 gene showed molecular responses in 80 percent of assessable patients who had a complete clinical response. After a median follow-up of 5.1 years, the actuarial 5-year progression-free survival for all patients was 59%, with a median progression-free survival of 6.1 years. Of the 57 patients who had a complete response, 40 remained in remission for 4.3 to 7.7 years. Hematologic toxicity was moderate, with no patient requiring transfusion or hematopoietic growth factors. Monoclonal antibodies for nonhematological malignancies: Targeted therapy against tumor-biological properties is an essential part of the individualized therapy concept in cancer. Next to risk-adapted strategies using conventional chemo- and/or endocrine therapies, antibody therapy has become an additional option.Trastuzumab The humanized MAb, trastuzumab (herceptin) is the first novel targeted therapy approved for routine clinical application in advanced breast cancer,[24] with HER2/ neu protein over expression as assessed by immunohistochemistry (IHC) and/or gene amplification as assessed by fluorescence in situ hybridization (FISH) in their tumors responding well to palliative trastuzumab therapy, either as single agent or in combination with chemotherapy. New combinations with endocrine therapy are currently being evaluated. Trastuzumab is generally well tolerated. So far, considerable cardiotoxicity was seen only in combination with doxorubicin. Thus, extensive cardio-monitoring is now performed in trials assessing further chemotherapeutic partners. Clinical trials looking at early-trastuzumab therapy in the adjuvant (e.g. HERA, BOND 006) or neoadjuvant (e.g. TECHNO) setting are still open for recruitment in Germany. Since only about 25 % of breast cancers, which are HER2/neu-positive, are eligible for trastuzumab, novel targeted therapeutics for the remaining HER2/neu-negative tumors are needed. Another therapeutic antibody, 2C4 (Pertuzumab, Omnitarg), is currently under clinical evaluation. It binds to a different epitope on HER2/neu than trastuzumab, and inhibits heterodimerization with other HER receptors. Phase I data showed that 2C4 is well tolerated and clinically active. Cetuximab Cetuximab is a recombinant human/mouse chimeric epidermal growth factor receptor (EGFR) MAb. It was approved by the US FDA in February 2004 to be used in combination with irinotecan for EGFR-expressing, metastatic colorectal cancer in patients who failed to improve with irinotecan-based chemotherapy. Cetuximab was also approved for administration as a single agent in the treatment of patients with EGFR-expressing, metastatic colorectal cancer who are intolerant to irinotecan-based chemotherapy.[25] A MEDLINE search[25] was conducted of articles published from 1976 to the present using the terms cetuximab, C225, IMC-C225, colon cancer, colorectal cancer, monoclonal therapy and target therapy. Abstracts presented at the American Society of Clinical Oncology annual meetings from 2000 to 2004 and the 2004 Gastrointestinal Cancers Symposium were reviewed and included as applicable. In a Phase III trial, cetuximab was administered to 329 patients with colorectal cancer who were irinotecan refractory and/or had failed to respond to oxaliplatin treatment. Partial response was achieved in 10.8% of patients who received cetuximab monotherapy and 22.9% of patients who received cetuximab plus irinotecan therapy (P = 0.007). The overall response rate in two Phase II trials using the conventional dosing regimen of cetuximab to treat EGFR-expressing, metastatic colorectal cancer that was refractory to irinotecan therapy ranged from 9% to 12%. The drug was well tolerated with proper administration precautions. Unfortunately, the role of immunohistochemistry for EGFR expression continues to be a poor predictor of patients who may benefit from cetuximab. Clinical studies of cetuximab in combination with radiation therapy and/or platinum in patients with squamous-cell head and neck cancer, as well as cetuximab in combination with various antineoplastic agents for non-small cell lung cancer and pancreatic cancer are going on. Cetuximab has shown considerable activity both as monotherapy and in combination with chemotherapy in the treatment of metastatic colorectal cancer that is resistant to chemotherapy. The future of cetuximab lies in its use in combination with antineoplastic agents and/or radiation therapy in the treatment of colorectal cancer, head and neck cancer, non-small cell lung cancer and pancreatic cancer. The lack of a predictive marker that would allow clinicians to select patients, who are most likely to benefit from cetuximab therapy, especially taking into consideration the high costs of this medication, remains a challenge. Bevacizumab Bevacizumab is a recombinant human MAb that inhibits the biological activities of VEGF, a protein involved in the neovascularization of malignant tumors. Studies have shown that bevacizumab has both cytostatic and cytotoxic effects, resulting in a reduction in tumor growth and increase in median survival time and time to tumor progression. Bevacizumab is available as an intravenous agent and carries FDA-approved labeling for use in the first-line treatment of metastatic colorectal cancer (CRC) in combination with fluorouracil-based chemotherapy. Bevacizumab has also yielded preliminary evidence of efficacy for breast, non-small-cell lung, pancreatic, prostate, renal and hepatic cancers, as well as for melanoma and acute myelogenous leukemia.[26] Bevacizumab increases survival when combined with irinotecan-based chemotherapy in first-line treatment of metastatic CRC. In a randomized phase II trial bevacizumab, 5-FU and leucovorin combination was compared with placebo plus FU/LV as first-line treatment in CRC.[27] Median survival was 16.6 months for the FU/LV/bevacizumab group and 12.9 months for FU/LV/placebo group. Median progression-free survival in the two groups was 9.2 vs 5.5 months. The response rate was 26% in the bevacizumab group and 15.2% in the FU/LV/placebo group. In a phase II study, the response rate and overall survival of pancreatic cancer patients who received gemcitabine with the recombinant humanized anti VEGF MAb bevacizumab was assessed. Fifty-two patients were enrolled at seven centers between November 2001 and March 2004. All patients had metastasis, and 83% had liver metastases. Eleven (21%) patients had confirmed partial response and 24 (46%) had stable disease. The 6-month survival rate was 77%. Median survival was 8.8 months; median progression-free survival was 5.4 months. The combination of bevacizumab plus gemcitabine is active in advanced pancreatic-cancer patients. Additional study is warranted. A randomized phase III trial of gemcitabine plus bevacizumab Vs. gemcitabine plus placebo is going on in pancreatic cancer and leukemia Group B.[28] In a recent study, the bevacizumab and erlotinib combination was evaluated in the treatment of metastatic clear-cell renal carcinoma,[29] which was effective and well-tolerated. The efficacy of the combination suggests that targeting of separate pathways critical to tumor growth and dissemination may achieve results superior to either drug as a single agent. In another study, bevacizumab in combination with capecitabine was assessed in breast cancer. Though there was a significant increase in response rate after addition of bevacizumab (19.8% Vs. 9.1%), this did not translate into improved progression-free survival and overall survival.[30] Panitumumab: Targets the epidermal growth factor receptor (EGFR), which is over-expressed in lung, breast, bladder, pancreatic, colorectal, kidney and head and neck cancers. Research has demonstrated that cancer cells can become dependent on growth signals mediated through EGFr for their survival. In preclinical research, panitumumab monotherapy has been shown to inhibit the growth of human tumors in mice.[31] Panitumumab is being evaluated in a comprehensive clinical program for several indications. The program currently includes clinical trials to evaluate panitumumab in renal, colorectal and non-small cell lung cancers. Mitumumab : Mitumumab is indicated in the treatment of SCLC, Melanoma and soft tissue sarcoma (CD11a).[32] Lymph°Cid- Epratuzumab is a MAb that targets CD22 protein found on β-cells. It has been tested in people with high- and low-grade NHL that has come back or is proving difficult to treat. It has been tested on its own and in combination with rituximab. Pertuzumab : This is a recombinant humanized monoclonal antibody (2C4) that binds to the extracellular domain II of the HER-2 receptor and blocks its ability to dimerize with other HER receptors. It represents a new class of targeted therapeutics known as HER dimerization inhibitors. A recent Phase I study[33] in patients with advanced breast cancer has shown that it is well tolerated and is clinically active, suggesting that inhibition of dimerisation may be an effective anticancer strategy. Conclusion After 30 years of development, therapy with MAbs has been recognized as a promising therapeutic tool. Its clinical use is most widespread in the field of oncology, where half of the agents approved for routine clinical use are employed and a large number of molecules are currently undergoing clinical trials. Monoclonal antibodies using human genes herald a new era in the treatment of cancer, autoimmune disease, graft rejection and infectious diseases and many products are being developed towards this end.References
Copyright 2006 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph06113t5.jpg] [ph06113t4.jpg] [ph06113t2.jpg] [ph06113t3.jpg] [ph06113t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}