 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Pharmacology, Vol. 38, No. 6, November-December, 2006, pp. 403-407 Research Paper Antiulcer effect of amlodipine and its interaction with H2 blocker and proton pump inhibitor in pylorus ligated rats Bhave AL, Bhatt JD, Hemavathi KG Department of Pharmacology, Medical College, Vadodara - 390 001. Gujarat Date of Submission: 14-Dec-2005 Code Number: ph06115 Abstract Objective: To study the interaction between a calcium channel blocker, amlodipine, and antiulcer agents, famotidine and omeprazole, in pylorus ligation-induced gastric ulcers in rats.Materials and Methods: Gastric ulcers were induced in albino rats by pyloric ligation as described by Shay et al . Effects of different doses of amlodipine, famotidine and omeprazole on volume, pH, acidity of gastric secretion and ulcer index were observed. In addition, the effects of low dose of amlodipine in combination with low dose of famotidine or omeprazole on the above parameters were studied. Results: Amlodipine (0.5 mg and 1 mg/kg, i.p.), famotidine (4 mg/kg, i.p.) and omeprazole (4 mg/kg, i.p.) produced significant antiulcer effects. Low doses of famotidine (1 mg/kg, i.p.), omeprazole (1 mg/kg, i.p.) and amlodipine (0.25 mg/kg, i.p.) did not alter the above parameters significantly. Combined administration of low dose of amlodipine (0.25 mg/kg) and famotidine (1 mg/kg) showed significant antiulcer effects, which were apparent from the reduction in volume of gastric acid secretion, acidity and ulcer index with simultaneous increase in the intragastric pH. Similarly, low dose of omeprazole (1 mg/kg) when combined with low dose of amlodipine (0.25 mg/kg) also showed significant antiulcer effects. Conclusion: Amlodipine produced significant antiulcer effects in pylorus-ligated model. Combination of low doses of amlodipine with low doses of either famotidine or omeprazole produced significant antiulcer effects. It is suggested that the patients who received amlodipine therapy for some other clinical conditions are less prone to develop peptic ulcers; and even if ulcers develop, they would require lower doses of antiulcer agents like famotidine and omeprazole. Keywords: Calcium channel blocker, famotidine, omeprazole Introduction Peptic ulcer disease is a major health problem with multifactorial etiology. The development of gastric ulcer occurs with acid and the breakdown of mucosal defence. Local mechanisms implicated in mucosal defence are; mucus-like alkaline secretions, mucosal hydrophilicity, rapid epithelial cell renewal, rich mucosal blood flow, mucosal sulphydryls and increased resistance of gland cells in deep mucosa to acid and peptic activity.[1] Calcium ions are involved in the regulation of acid secretion in the stomach[2],[3] and has been considered as a serious contender responsible for the development of various types of ulcers.[4] Calcium influx plays an important role in stimulation-secretion coupling in mammalian oxyntic cells, an effect that can be inhibited by calcium channel blockers.[5] Moreover, calcium channel blockers exert an inhibitory effect on histamine-, gastrin-, carbachol- and cyclic-AMP-induced stimulation of gastric acid secretion.[6] So, there is a possibility that calcium channel blockers, which act by reducing the transmembrane calcium influx, may influence the secretion of hydrochloric acid in the stomach and thus may have a protective effect against gastric ulcers. The gastroprotective effects of calcium channel blockers, viz., verapamil, nifedipine and diltiazem, have been reported.[7],[8],[9] Nifedipine, verapamil and diltiazem have been reported to potentiate the antiulcer and antisecretory effects of famotidine at low doses.[10] Amlodipine, a long- acting calcium channel blocker is at present widely used in clinical practice for the management of various cardiovascular disorders. It is likely that because of its long action, the gastric protective effects of amlodipine may differ from that of other calcium channel blockers. But, at present, the data regarding the interaction of amlodipine with various antiulcer agents are not available. Therefore, the present study was undertaken to evaluate the effects of the slow- and long- acting calcium channel blocker, amlodipine, on gastric secretion and other parameters as well as its interaction with a H 2 -blocker, famotidine, and a proton-pump inhibitor, omeprazole, in pylorus-ligated gastric ulcer model in rats.
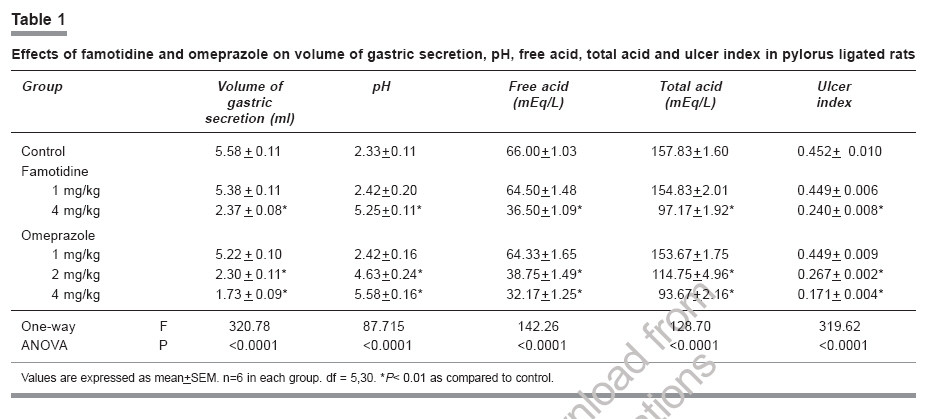
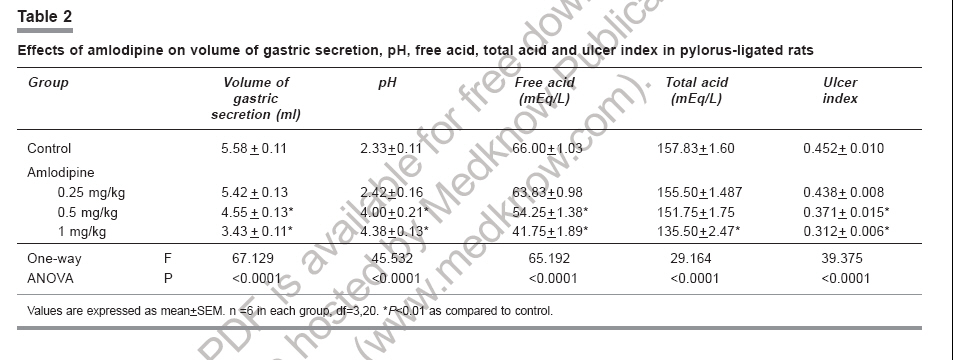
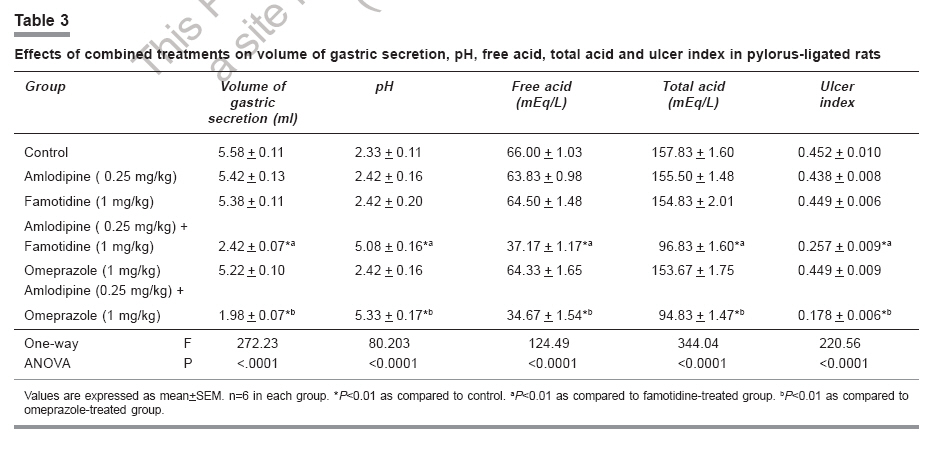
Materials and Methods Wistar strain albino rats of either sex weighing 200-250 g were kept in the department animal house at room temperature (25°C-30°C) and were fed on regular laboratory diet with water ad libitum . Rats were divided into various groups (n=6 in each group) viz., Control, dimethylsulphoxide (DMSO) (vehicle) treated, famotidine treated (1 and 4 mg/ kg), omeprazole treated (1, 2 and 4 mg/kg), amlodipine treated (0.25, 0.5 and 1 mg/kg) and finally a combination treatment of amlodipine (0.25 mg/kg) with famotidine (1 mg/kg) and amlodipine (0.25 mg/kg) with omeprazole (1mg/kg). All drugs were administered intraperitoneally ( i.p.) 1 h prior to pyloric ligation (PL), except amlodipine which was given 4 h prior to PL and two groups treated with DMSO - one receiving DMSO 4 h prior to PL and the other 1 h prior to PL. Control group received normal saline. The volume of all the above injections varied between 0.2 to 0.4 ml. Pyloric ligation was performed as described by Shay et al .[11] Rats were fasted for 36 h prior to the surgical procedure and kept in raised mesh-bottomed cages to avoid coprophagy. Under urethane anesthesia (80 mg/100 g, i.p.) the abdomen was opened by a small midline incision below the xiphoid process. The pyloric portion of the stomach was identified, slightly lifted out and ligated, avoiding traction to the pylorus or damage to the blood supply. The stomach was then replaced carefully and the abdominal wall closed by interrupted sutures. Animals were deprived of both food and water during the postoperative period and were sacrificed at the end of 19- 20 h after the operation. The stomach was dissected out as a whole by passing a ligature at the esophageal end. The stomach was separated from the surrounding tissues and organs and thus brought out as a whole alongwith its contents. The contents were subjected to centrifugation (3000 rpm for 10 min) and then analyzed for volume, pH, and free and total acidity. The pH was estimated using Indikrom pH strips (Glaxo India Limited, India) with pH ranges of 2.0-4.5 and 5.0-8.5 with a difference in range of 0.5. Free acidity and total acidity were estimated by titrating 1 ml of the centrifuged sample with 0.01 N NaOH, using Topfer's indicator and phenolpthalein indicator, respectively. Acidity was expressed in clinical units, i.e the amount of 0.01 N NaOH base required to titrate 100 ml of gastric secretion. For estimation of ulcer index, the stomach was cut open along the greater curvature and the inner surface was examined for ulceration with the help of a simple dissecting microscope. Usually, circular lesions were observed but, sometimes, linear lesions were also seen. The ulcer index was calculated by using the formula.[12] Drugs used Fresh solutions of amlodipine besylate (Intas Pharmaceuticals, Ahmedabad), famotidine (Sun Pharmaceutical Industries, Vadodara) and omeprazole (Cipla, Mumbai) were prepared daily in DMSO. Statistical analysis All data are expressed as mean ± SEM. For comparison amongst different groups, post hoc one-way ANOVA was performed. A P value less than 5% ( P < 0.05) was considered to be statistically significant. Results Effects of DMSO (vehicle) The DMSO administered prior (4 h or 1 h) to pylorus ligation did not produce any significant change in the volume of gastric secretion, pH, free acid, total acid and ulcer index as compared to the control values. Effects of famotidine Famotidine in a dose of 1 mg/kg did not produce any significant change in any of the parameters studied. [Table - 1] However 4 mg/kg famotidine produced significant decrease in the volume of gastric secretion, free acid, total acid and ulcer index alongwith significant ( P < 0.01) increase in the pH as compared to the control. [Table - 1] Effects of omeprazole Omeprazole in a dose of 1 mg/kg produced a significant ( P < 0.05) decrease in the volume of gastric secretion as compared to the control value without significantly modifying the pH, free acid, total acid and ulcer index values. [Table - 1] Whereas, omeprazole in doses of 2 mg/kg and 4 mg/kg produced significant ( P < 0.01) dose-dependent increase in pH value and significant dose-dependent decrease in other parameters, as compared to the control values. [Table - 1] Effects of amlodipine Amlodipine in a dose of 0.25 mg/kg did not modify any of the parameters significantly. However, in doses of 0.5 mg/kg and 1 mg/kg, it produced a dose-dependent decrease in the volume of gastric secretion, free acid, total acid and ulcer index and a significant increase in the pH values, as compared to the control values. [Table - 2] Effects of combined treatments Combined treatment consisting of famotidine (1 mg/kg) with amlodipine (0.25 mg/kg) produced a significant ( P < 0.01) decrease in the volume of gastric secretion, free acid, total acid and ulcer index with a significant increase in the pH values, as compared to the control values as well as to the groups that received either famotidine or amlodipine alone. [Table - 3] Combination of omeprazole (1 mg/kg) and amlodipine (0.25 mg/kg) also produced a significant ( P < 0.01) decrease in the values of all the parameters, with a significant increase in the pH values, as compared to the control values as well as to the groups that received either omeprazole or amlodipine alone. [Table - 3] Discussion The etiology of peptic ulcer is unknown in most of the cases, yet it is generally accepted that it results from an imbalance between aggressive factors and the maintenance of mucosal integrity through the endogenous defense mechanisms.[13] To regain the balance, different therapeutic agents are used to inhibit the gastric acid secretion or to boost the mucosal defense mechanisms by increasing mucus production, stabilizing the surface epithelial cells or interfering with the prostaglandin synthesis.[14] The causes of gastric ulcer after pyloric ligation are believed to be due to stress-induced increase in gastric hydrochloric acid secretion and/or stasis of acid. According to Shay et al ., the volume of secretion is also an important factor in the formation of ulcer due to exposure of the unprotected lumen of the stomach to the accumulating acid. Famotidine, a competitive antagonist of H 2 -receptor, is capable of reducing over 90% of basal and nocturnal secretion of gastric acid and that stimulated by food, histamine, gastrin, cholinomimetic drugs and vagal stimulation.[15] Famotidine reduces acidity and volume of gastric secretion by blocking the effect of histamine. It can also reduce the gastrin and the vagus nerve- mediated secretion to some extent.[10] Famotidine exerts its antisecretory effect by inhibiting the histamine-induced cyclic-AMP-dependent pathway.[16] The proton pump inhibitor omeprazole produces small and inconsistent changes in the volume of gastric secretion and in the secretion of pepsin, but it does not affect gastric motility. It irreversibly inhibits the gastric acid (proton) pump which is the final common pathway for acid secretion in response to all varieties of stimuli. It produces virtual anacidity in vivo. In the present study, therapeutically equivalent doses of amlodipine (0.5 mg and 1 mg/kg) produced significant decrease in the volume, free acidity and total acidity of the gastric secretion alongwith a significant protective effect against gastric ulceration induced by pylorus ligation. A lower dose of 0.25 mg/kg did not produce any significant alteration in the parameters studied. Gastric acid secretion is under vagal control and overactivity of vagus also contributes to ulcer formation.[9] Vagal stimulation increases acetylcholine that acts directly on the muscarinic receptors on parietal cells and secretes hydrochloric acid through a calcium-dependent pathway.[16] Mandal et al .,[10] have shown that the protective effect of verapamil and nifedipine against gastric ulcer may partly be due to inhibition of this calcium-dependent pathway. The gastric antisecretory effect of amlodipine may be due to a similar mechanism. Amlodipine may also act by antagonizing the injurious effects of histamine and other biogenic amines on the capillaries of gastric mucosa, as suggested for nifedipine and verapamil.[8],[10] Verapamil has been reported to inhibit mast-cell degranulation,[9] acid secretion[17],[18] and gastric motility. Koo et al .,[19] reported antiulcer activity of verapamil in stress-induced ulcer formation based upon its action on the preservation of mucus. Jain et al .,[8],[9] and Jain and Santani,[20] using three calcium channel blockers, viz ., verapamil, diltiazem and nifedipine, reported a decrease in gastric acid secretion and a rise in the TC/PR ratio { TC = total carbohydrate content of gastric juice, PR = total protein content of gastric juice }, indicating improved mucus activity, which in turn strengthens mucosal barrier; as possible mechanisms of antiulcer activity of all the three calcium channel blockers. Therefore, it seems likely that amlodipine may be acting by the similar mechanisms as reported above. A role for reactive oxygen metabolites, free radicals and nitric oxide has been suggested in the pathogenesis of gastric ulcer.[21],[22],[23],[24] Recently, Ding and Vaziri [25] reported that prototypes of dihydropyridines like nifedipine up-regulate the nitric oxide (NO) system in endothelial cells suggesting, in part its different biological properties. Amlodipine has also been reported to increase NO release from the coronary microvasculature of failing human myocardium.[26] Thus, it is tempting to suggest that the amlodipine-induced protective effects in pylorus-ligated gastric ulcers could be in part also mediated through either a decrease in free-radical generation or an increase in nitric oxide production. Further study is necessary to identify the role of amlodipine on the above factors. In the present study, low doses of either famotidine (1 mg/kg), omeprazole (1 mg/kg) or amlodipine (0.25 mg/kg) did not produce any antiulcer effect. Higher doses of amlodipine (0.5 mg and 1 mg/kg) produced a significant protective effect against experimental gastric ulceration in rats. However, a combination of low dose (0.25 mg/kg) of amlodipine with low dose (1 mg/kg) of famotidine produced a significant antiulcer effect. Similarly, a low dose of amlodipine (0.25 mg/kg) combined with a low dose of omeprazole (1 mg/kg) also produced significant antiulcer activity. It is likely that amlodipine like other dihydropyridine calcium channel blockers[8],[10],[20] may have antiulcer activity through multiple (2 or more) separate mechanisms, which are different from the mechanisms of famotidine and omeprazole. Hence, simultaneous administration of low doses of amlodipine with either famotidine or omeprazole may produce significant antiulcer effects, as reflected by the reduction of volume of gastric secretion, acidity and ulcer index. From the present investigation, it may be concluded that amlodipine produced a significant protective effect against gastric ulceration and also produced significant antiulcer effects when used in combination with famotidine and omeprazole. It is to be studied whether doses of famotidine and omeprazole could be reduced for the management of peptic ulcer in patients who are on amlodipine therapy. References
Copyright 2006 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph06115t3.jpg] [ph06115t1.jpg] [ph06115t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}