 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Pharmacology, Vol. 38, No. 6, November-December, 2006, pp. 429-431 Research Letter Adverse cutaneous drug reactions: A one year survey at a dermatology outpatient clinic of a tertiary care hospital Chatterjee S, Ghosh AP, Barbhuiya J, Dey SK Department of Pharmacology, Institute of Postgraduate Medical Education and Research, 244 B, AJC Bose Road, Kolkata-700020 Code Number: ph06121 Adverse cutaneous drug reactions (ACDR) form an important clinical entity in dermatology practice and the severity of such reactions vary from mild to fatal ones. Although such cutaneous reactions are common, comprehensive information about their incidence, severity and ultimate health effects are often not available. Data regarding the safety profile of a drug prior to marketing is essentially based on preclinical and clinical studies and the later involve only a limited number of subjects. However, when drugs are marketed and used extensively, new adverse events are unearthed. This in fact re-emphasizes the utility of an efficient pharmacovigilance system that could generate valuable data for health care deliverers and their beneficiaries. The incidence of ACDR in developed countries range from 1-3% among in patients[1],[2] whereas in developing countries like India some studies peg it to 2-5% of the inpatients,[3],[4],[5],[6],[7] but there is lack of comprehensive data amongst out patients. Inadequacy of data could be attributed to reasons like, diagnostic dilemmas and lack of awareness to report. Therefore the objectives of the present study were:
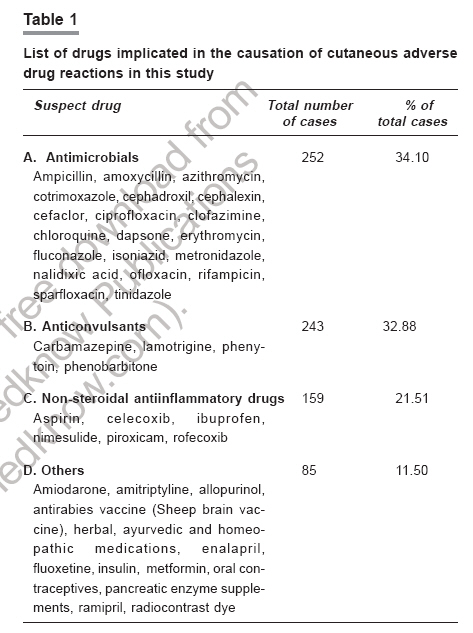
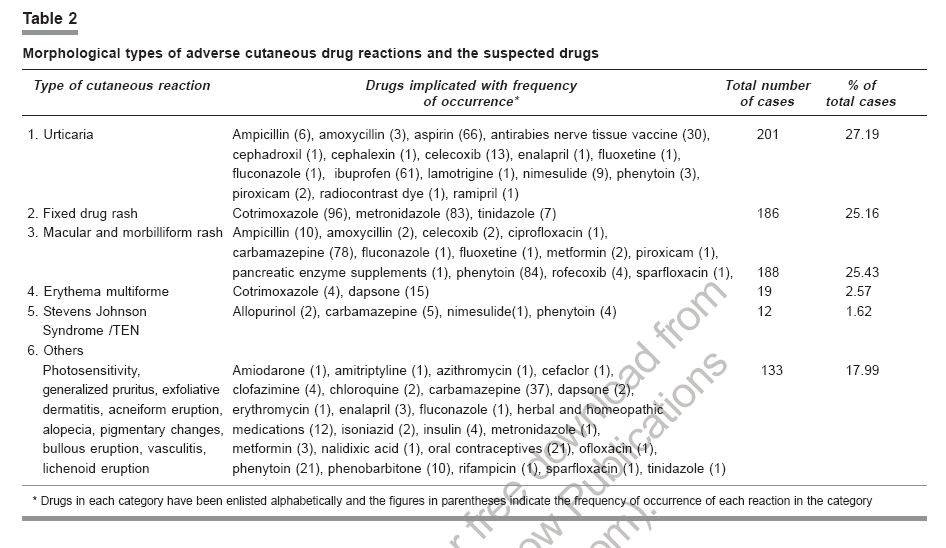
The study was a prospective, observational study carried out in the Dermatology OPD of N.R.S. Medical College and Hospital, Kolkata, India with approval from the Institutional Ethics Committee. All patients who attended the Dermatology OPD of the hospital from 1st May 2002 to the 30th April 2003 were screened. Suspected cases of ACDR were independently assessed by two Dermatology consultants of the department and subsequently causality assessment was done by a Pharmacologist using WHO guidelines.[8] Only those cases where the causality was certain, probable/likely were recorded. Detailed clinical history, drug history and relevant information like onset of the reaction, its duration and temporal association with drug intake if any, enlistment of all drugs taken preceding the onset of reaction, past history of drug rashes, reports of relevant laboratory investigations undertaken to arrive at a clinical diagnosis were recorded. All the above information were recorded in a predesigned ADR reporting form. The data was compiled on a Microsoft excel sheet and subjected to descriptive statistical analysis. A total of 27,726 patients attended the Dermatology OPD during the study period of one year. The incidence of ACDR was 2.66 % (739) of the total patients screened. The mean age of occurrence was 26.74 ±9.39 year in females and 26.81 ±10.22 year in males. Female patients constituted 61.16 % of the total cases. A study[7] conducted in a tertiary care center in South India had revealed that the mean age of ACDR was 37.06 year and the female-male ratio being 0.87:1. The common offending drug groups as depicted in [Table - 1] were antimicrobials (34.10%), anticonvulsants (32.88%), antiinflammatory drugs (21.51%). Other less frequent ones were antipsychotics, antidepressants, antihypertensives, oral contraceptives, antidiabetics, insulin, vaccines, radiocontrasts, pancreatic enzyme supplements, homeopathic and ayurvedic preparations. The most common offending drugs were carbamazepine (16.23%), phenytoin (15.15%) and cotrimoxazole (13.53%), however antimicrobials were the most common drug group implicated. The most common morphological varieties of the reactions were urticaria (27.19%) fixed drug rashes (25.16%) and macular and morbilliform eruptions (25.43%). The drugs implicated in these reactions with the frequency of occurrence are enlisted in [Table - 2]. A recent study conducted in southern India has reported that the most common observed reactions were fixed drug eruptions (31.1%) and maculopapular rashes (12.2%).[7] Analysis of the data shows that NSAIDs were the most common drug groups (151/201) implicated in urticarial lesions. Antimicrobials were the only class of drugs that caused FDRs. Anticonvulsants (162/188) were the common offenders in macular, maculo-papular and morbilliform rashes category. Of the 12 cases of suspected Stevens Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis (TEN) the drugs implicated were carbamazepine (5), phenytoin (4), allopurinol (2) and nimesulide (1). Analysis of the outcome of such reactions reveal that there was clinical improvement and abatement of reactions within 7 days of dechallenge in 87% of the cases, while delayed improvement was observed in 11% cases. There were 12 cases (1.62%) of severe ACDR (SJS and TEN) and all these were admitted for treatment with 5 deaths (0.67%) reported. In the causality assessment using WHO guidelines, there were 541 probable and 198 certain cases. History of atopy was present in 45% of cases of urticarial and morbilliform rashes which could be considered as a predisposing factor for the reactions.[9] As this hospital was a referral centre in Kolkata for administration of antirabies (sheep brain) vaccine a large number of cases with urticaria and angioedema were reported however it is very rarely used in clinical practice presently. Since most of the patients attending the OPD of this hospital belong to relatively poor socio-economic status the pattern of drug usage amongst them is mostly restricted to drugs that are supplied free of cost from the hospital. As a consequence, the suspect drugs were mostly from the hospital OPD supply list. This was an important limitation of this study as the suspect drug data generated from this study may not be truly reflective of the pattern in other tertiary care centres catering to patients of higher socio-economic status. This study reveals that the incidence of drug induced adverse skin reactions at a dermatology out patient setting is 2.6%. Since previous studies were principally done amongst hospitalized patients this study provides data about the magnitude of this clinical entity in an out patient setting. Analysis of the data shows that urticaria and fixed drug rashes were the most common morphological reaction types. Carbamazepine and phenytoin were the most common offenders. Despite the limitations of spontaneous reporting of adverse drug reactions, it can still be considered as an effective tool in Pharmacovigilance. Only if clinicians recognize and foster a culture for reporting such reactions to regulatory authorities drug safety measures can be taken. Acknowledgments The present study was a UGC sponsored minor research project. The authors are grateful to all the administrative, teaching, non-teaching staff and postgraduate students of the Dermatology Dept of the hospital for their support. References
Copyright 2006 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph06121t1.jpg] [ph06121t2.jpg] |
| |||||||||

{kind=link}
{kind=link}