 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
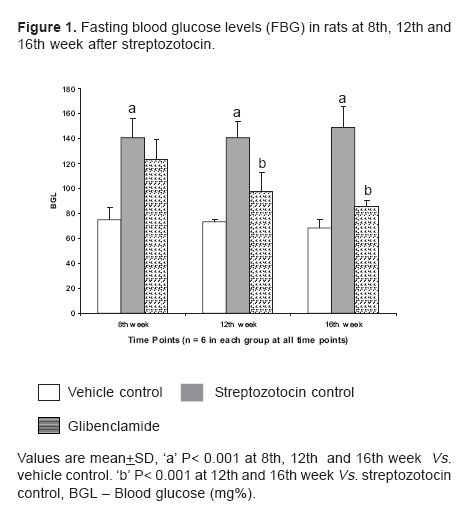
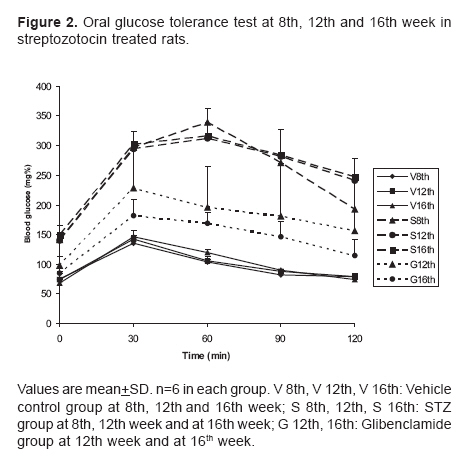
Indian Journal of Pharmacology, Vol. 38, No. 6, November-December, 2006, pp. 432-433 Research Letter A split dose regimen of streptozotocin to induce diabetes in a neonatal rat model Marathe PA, Parekar RR, Shinde SP, Rege NN Department of Pharmacology and Therapeutics, Seth G.S. Medical College and K.E.M. Hospital, Parel, Mumbai - 400 012 Code Number: ph06122 Streptozotocin (STZ) is used in rats within 5 days of birth in doses ranging from 80 to 100 mg/kg to create features simulating type 2 diabetes (known as n0-n5 models). [1],[2],[3] Most of the beta cells in neonates are destroyed by STZ, but they gradually regenerate to about half the original mass. The animals exhibiting blood glucose levels above 100 mg% are considered as diabetic.[4] By varying the administration time of STZ, one can obtain hyperglycemia of differing severity depending upon the extent of beta-cell damage and regeneration.[2],[5] Susceptibility of rats to STZ varies with species, strain, sex, age and nutritional state of the animals, and all the STZ-treated animals do not develop hyperglycemia.[6] Variations in blood glucose levels, high mortality (30-50%) due to STZ toxicity and lack of response to oral hypoglycemic drugs are the drawbacks of n0 and n5 models.[2],[5],[7] In addition, there is no documentation of the number of excluded animals which failed to show desired hyperglycemia. A study by Portha et al , in 1974 has shown that a split dose of STZ injected over two consecutive days (day 0 and 1) after birth induces hyperglycemia and decreases pancreatic insulin stores by day 5 as compared to a single dose injection.[1] In this study the authors did not investigate the blood glucose and insulin levels beyond 3 weeks. Such a split dose regimen has not been used by any other researcher.[3] Hence, we decided to test the efficacy of a split dose regimen of STZ to develop a neonatal diabetes model. After obtaining the permission of the Animal Ethics Committee, seven batches of newborn, Wistar rat pups (n=54) consisting of six to eight per batch were taken up. STZ was administered to 46 neonates on the 2nd and 3rd postnatal day in the dose of 50 mg/kg/day intraperitoneally, and 0.3 ml of vehicle (citrated buffer) was administered to eight neonates. After 28 days, the neonates were weaned. Fasting blood glucose (FBG) and oral glucose tolerance test (OGTT) were carried out at 8 weeks. The latter was in response to 2 g/kg oral glucose. Two millilitre of blood was collected from the retroorbital sinus for measuring FBG using semi-autoanalyser (Erba-CHEM 5 plus, Transasia Biomedical Ltd., India. For OGTT, blood sugar was estimated taking one drop of blood (65 µl) from the retroorbital sinus at each time point, i.e., at ½, 1, 1 ½, and 2 h, with Accucheck Active GlucometerTM (Roche Diagnostics Corporation, Indianapolis, USA). Our animal laboratory range of FBG for 8 week old normal rats is 69.51±5.60 mg% (60 - 80 mg%). In the present study, in animals with FBG of ≥ 90 mg% at 8 weeks, responses to oral glucose load and mortality were recorded. The blood glucose levels were compared using one-way ANOVA with post hoc Tukey's test ( P < 0.05). The mortality in the STZ group was 15.22% (7/46) whereas in the vehicle treated group it was 25% (2/8). The deaths were observed within the 1st and 2nd week of STZ injection. (In the STZ group, five animals died in the 1st week and two animals died in the 2nd week, while in the vehicle treated group one animal died in the 1st week and the other in the 4th week). Thirty-five out of 39 rats (89.74%) developed hyperglycemia in the range of 100-160 mg%. The average FBG was 119.94±17.93 mg%. Out of the six batches that were administered STZ, five showed uniform levels of hyperglycemia (102-130 mg%). However, only one batch showed a higher level of 153.04±9.21 mg%. The FBG of the vehicle treated group was found to be 75.33±8.91. Twelve hyperglycemic rats from the STZ treated group and six from the vehicle group were observed for a further period of 8 weeks. Six of these 12 STZ treated rats were administered glibenclamide in a dose of 0.5 mg/kg orally once daily, to evaluate the effect of the oral hypoglycemic agent on FBG and OGTT. In all these rats, FBG and OGTT were reassessed at the end of the 12th and the 16th week. The hyperglycemia in the STZ group sustained even at the 12th week and the 16th week. All the six animals survived upto the 16th week. However, in rats treated with glibenclamide, significantly lower FBG levels were seen ( P < 0.001). [Figure - 1] The STZ and vehicle groups exhibited significant difference with respect to OGTT ( P < 0.01). All the six animals which were administered glibenclamide survived up to the 16th week and showed significantly improved tolerance to the given glucose load at all time points as compared to the STZ group ( P < 0.01). [Figure - 2] In this study, the mortality rate in the control group was comparable to that reported by other researchers (10-30%) [2] whereas a remarkable reduction was seen in the mortality induced by STZ (30-50% in n 0, n 5 models).[2],[5] Moreover, the extent of hyperglycemia remains comparable to that seen with single dose of STZ. Incidence of development of hyperglycemia was 90% and variations in FBG levels among the different batches were less, indicating uniformity of response. The low mortality and the moderate hyperglycemia following the split dose regimen may be the result of low doses and administration timings of STZ. This regimen probably leads to beta cell damage in a graded fashion, sparing some beta cell mass, and allows time for regeneration in between the two injections. The measurements of the insulin levels would have clarified the extent of destruction of the beta cells of the pancreas by STZ in the current study. In addition to the graded destruction of pancreatic beta cells, enhancement of glucose uptake into the skeletal muscle, changes in transporters, alterations in the sensitivity of peripheral tissues and decreased oxidative stress could have been the other possible mechanisms responsible for the mild to moderate levels of hyperglycemia observed in the study. The rats given a split dose of STZ maintained hyperglycemic status and abnormal glucose tolerance till the 16th week of life. Glibenclamide, a standard oral hypoglycemic agent, exhibited antihyperglycemic response at both 12 and 16 weeks, indicating that the model is suitable for the evaluation of antidiabetic drugs. Thus, induction of diabetic model in neonatal rats using a split dose regimen of STZ is a refinement of previous models and offers the following advantages:
Though the complete characterization of the model remains to be done, we wish to share the data regarding hyperglycemia and OGTT with other researchers, especially those working in a small laboratory set-up with minimum resources, and make them aware of a technique which is reliable and economical. References
Copyright 2006 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph06122f2.jpg] [ph06122f1.jpg] |
| |||||||||

{kind=link}
{kind=link}