 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Pharmacology, Vol. 39, No. 1, January-February, 2007, pp. 20-24 Research Paper In vivo pharmacodynamic interaction between pipecuronium and certain H2 blockers Trivedi HR, Tripathi CB, Bhatt JD, Shah KK, Hemavathi KG Department of Pharmacology, Medical College, Baroda Date of Submission: 26-Apr-2006 Code Number: ph07004 Abstract Objective: To investigate the pharmacodynamic interaction of H2 -receptor antagonists (i.e., famotidine and roxatidine acetate) with a neuromuscular blocker, pipecuronium using sciatic nerve stimulated gastrocnemius preparation of rats in vivo .Materials and Methods: The dose-response curve of pipecuronium (10-50 mg/kg i.v.) was elicited and the dose (ID50; 26.89 mg/kg i.v.) required to cause 50% of blockade of basal contractile twitch response was calculated. Benzyl alcohol (0.9 % v/v), famotidine (0.5, 2.0, 5.0 mg/kg i.v.) or roxatidine acetate (0.05, 0.2, 0.5 mg/kg i.v.) were administered 30 min prior to pipecuronium administration and their effects were studied on the dose-response curve of pipecuronium. Results: Famotidine did not alter the basal contractile twitch responses but with a dose of 2 mg/kg it significantly decreased, while with 5 mg/kg, it significantly increased the ID50 of pipecuronium. At higher dose (5.0 mg/kg) it significantly increased the time required for the onset of blockade without affecting the other parameters. Roxatidine acetate (0.2, 0.5 mg/kg) by itself produced significant neuromuscular blockade but did not alter the ID50 of pipecuronium, while with higher dose (0.5 mg/kg) it significantly decreased the same. Roxatidine (0.05 and 0.2 mg/kg) significantly increased the time required for onset of pipecuronium-induced neuromuscular blockade. At varying doses roxatidine also significantly increased the time required for peak effect and the recovery from the paralysis. Conclusion: Compared to roxatidine, famotidine produced less pharmacodynamic drug interaction with pipecuronium in rats. Such an interaction should be explored in clinical practice. Keywords: Drug interaction, H2 receptor blockers, nerve-muscle preparation, non-depolarizing neuromuscular blocker. Introduction Aspiration of gastric contents in anesthetic practice is associated with a high mortality and morbidity especially during emergency procedures.[1] A gastric pH < 2.5 and a volume> 25 mL is critical to the pulmonary damage in adult patients[2] but low volume pulmonary aspirates (0.3 mL/kg) with pH less than one have resulted in high (90%) mortality rates in rats.[3] H 2 -antagonists, antacids and drugs that modify gastric emptying have been used to reduce pulmonary injury that follows aspiration of gastric contents.[4] H 2 antagonists[5],[6] are the preferred preanaesthetic for prevention of acid aspiration syndrome. Neuromuscular blocking drugs, which promote skeletal muscle relaxation, are administered routinely for tracheal intubation, during major surgical as well as minor procedures like scopies. However, there is a potential for interaction with neuromuscular blockers. Omeprazole[7] and cimetidine[8] have been reported to enhance the action of neuromuscular blockers. Cimetidine has been shown to prolong the duration of action of vecuronium.[8] At high concentration, nizatidine and ranitidine potentiated the neuromuscular blocking activity of d-tubocurarine, while a reverse action was noted at lower concentration.[9] Famotidine did not alter the neuromuscular blockade produced by vecuronium.[10] Roxatidine, by itself caused blockade of neuromuscular transmission apart from potentiating the neuromuscular blockade induced by d-tubocurarine, pancuronium and aminoglycoside-kanamycin.[11] In view of the diverse reports, the present study was planned to examine the interaction of H 2 antagonists famotidine and roxatidine acetate with the long acting neuromuscular blocker, pipecuronium, using the sciatic-gastrocnemius nerve-muscle preparation of rat in vivo . Materials and Methods Drugs Benzyl alcohol (Sarabhai Chemicals, Baroda); famotidine (Intas Pharmaceuticals Ltd., Ahmedabad); pipecuronium (Themis Pharmaceuticals, Mumbai); roxatidine acetate hydrochloride (Hoechst India Limited, Mumbai). Benzyl alcohol (vehicle of famotidine) was diluted in saline and equivalent of dilution was prepared as per its concentration present in stock solution of famotidine injection (i.e., 0.9 % v/v of benzyl alcohol in 10 mg/mL of famotidine injection). Contents of the ampoules of famotidine (10 mg/mL) and pipecuronium (2 mg/mL) were diluted in saline and roxatidine acetate powder was dissolved in saline. Appropriate fresh saline dilutions of all the drugs were prepared on the day of the experiment. All the drugs/vehicle (including pipecuronium) were administered intravenously, 30 min prior to pipecuronium. Albino rats (250-400 gm) of either sex were fasted for 24 hour prior to the experiment. Under urethane (1.25 g/kg ip) tracheotomy was done and artificially ventilated (8-10 mL/kg volume of air with 50-70 strokes per minute) using, rodent respiratory pump. The external jugular vein was cannulated for drug administration. The gastrocnemius-sciatic muscle-nerve preparation was set up as described by Mishra et al.[12] The body temperature was maintained using homoeothermic surgical table and overhead lamp. The preparation was allowed to stabilize for 30 min before starting the experiment. With the student′s physiograph, (Bio Device, Ambala) the sciatic nerve was stimulated (2V, 0.1 Hz and 0.2 ms) using a bipolar electrode (Dastre′s electrode) stimulator and the baseline contractile twitch responses were recorded. Pipecuronium 10 mg/kg was administered i.v. every 30 sec till complete paralysis (i.e., till complete inhibition of the basal contractile twitch response). Dose required to produce 50% paralysis (ID 50 value) was calculated by the best fitting regression line. Effects of highest doses (0.4 mL of benzyl alcohol 0.9% v/v (vehicle for famotidine), famotidine (0.5, 2 and 5 mg/kg) and roxatidine acetate (0.05, 0.2 and 0.5 mg/kg) were studied in the nerve-muscle preparation using separate group of six animals each. For each drug, the effect of a single dose was studied for 3 min. The following parameters of neuromuscular blockade were studied:
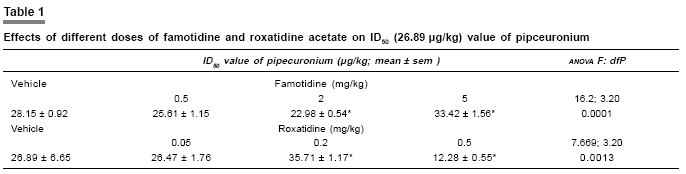
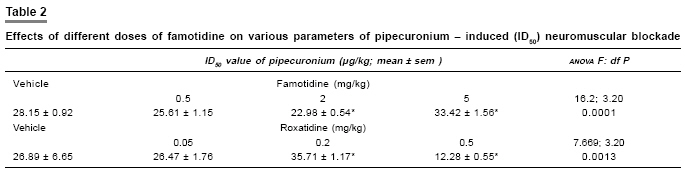
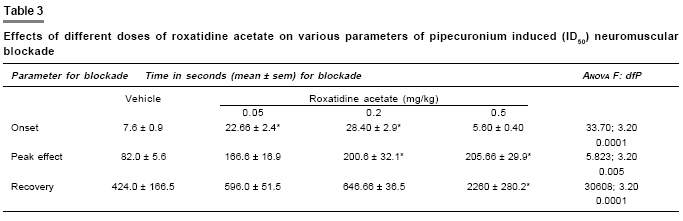
Statistical analysis Results were expressed as mean ± SEM. For comparison of ID 50 values and percentage of neuromuscular blockade and other values amongst different groups, one way anova with post hoc test was employed. P < 0.05 was considered to be statistically significant. Results Effects of pipecuronium, famotidine and roxatidine acetate on the basal contractile twitch response of sciatic nerve stimulated gastrocnemius preparation Pipecuronium produced a dose-dependent inhibition of the nerve stimulated basal contractile twitch responses of the muscle. Both the vehicle (benzyl alcohol) and famotidine did not produce any significant effect on the preparation (data not shown). Roxatidine acetate (0.2 and 0.5 mg/kg) significantly inhibited the basal twitch response (i.e., 16.63 ± 1.84% and 20.23 ± 4.43%, respectively). The ID 50 (26.89 mg/kg) dose of pipecuronium produced a 51% of inhibition of the nerve stimulated contractile twitch responses. Effects of famotidine and roxatidine acetate on neuromuscular blockade produced by ID 50 (26.89 µg/kg) dose of pipecuronium Pretreatment with either vehicle or lower dose (0.5 mg/kg) of famotidine did not modify the blockade produced by pipecuronium or its ID 50 value [Table - 1]. However, intermediate dose (2 mg/kg) produced leftward shift of the dose response curve of pipecuronium with a significant decrease in ID 50 value, while higher dose (5 mg/kg) produced an opposite effect [Table - 1]. Roxatidine acetate in lower dose (0.05 mg/kg) did not significantly modify the neuromuscular blockade induced by pipecuronium or its ID 50 value Table - 1. However, intermediate dose (0.2 mg/kg) of roxatidine acetate produced parallel rightward shift of the dose response curve of pipecuronium with a significant increase in the ID 50 and the higher dose (0.5 mg/kg) produced a parallel leftward shift of dose response curve with a significant decrease in the ID 50 Table - 1. Effects of famotidine and roxatidine acetate on different parameters of neuromuscular blockade produced by the ID 50 (26.89 µg/kg) dose of pipecuronium Famotidine (0.5 and 2 µg/kg) did not modify the time required for the onset, development of peak effect and recovery from the neuromuscular blockade produced by ID 50 dose of pipecuronium (26.89 µg/kg; Table - 2). However a higher dose (5 mg/kg) significantly increased the time required for onset of neuromuscular blockade produced by ID 50 dose of pipecuronium without modifying the time required for the peak effect and recovery from the blockade Table - 2. Roxatidine acetate (0.05 and 0.2 mg/kg) significantly increased the time required for the onset of neuromuscular blockade and at 0.2 and 0.5 mg/kg doses significantly increased the time required for the development of peak blockade produced by ID 50 dose of pipecuronium (26.89 µg/kg). Roxatidine acetate (0.5 mg/kg) significantly increased the time required for the peak effect and recovery from the neuromuscular blockade produced by ID 50 dose of pipecuronium [Table - 3]. Discussion Pipecuronium (50 mg/kg) produced complete blockade of the twitch responses of the sciatic nerve stimulated gastrocnemius preparation, which is in line with previous experimental[12] and clinical studies.[13] Benzyl alcohol (vehicle) did not modify any of the parameters studied. Mishra et al[14] reported that famotidine failed to alter the steady state paralysis produced by non-depolarising (e.g., atracurium and gallamine) as well as depolarising (e.g., succinylcholine) blockers in vivo in rats. Similar results were obtained with low dose (0.5 mg/kg) famotidine in the present study involving non-depolarising blocker. However, the intermediate dose significantly enhanced pipecuronium-induced paralysis (i.e., decreased ID 50 ) without modifying the other parameters. Famotidine has been reported to potentiate the neuromuscular blockade produced by d-tubocurarine, pancuronium and aminoglycoside antibiotics.[11] This potentiation of could be either (i) due to antagonism of calcium ions at presynaptic site as reported for the H 2 antagonists cimetidine and ranitidine[10] or (ii) due to their ion channel blocking effect.[11] Higher dose (5 mg/kg) of famotidine significantly antagonized pipecuronium-induced paralysis (increase in ID 50 ; rightward shift) with significant increase in the time required for onset of paralysis without modifying the time required for peak effect and recovery from the paralysis. The antagonism by famotidine may be attributed to its weak anticholinesterase activity,[15] as reported for ranitidine in vivo .[16],[17] Thus it is likely that the rightward shift of dose response curve of pipecuronium could be due to delay in onset of paralysis produced by famotidine. These results are in contrast to those reported by Mishra et al[10] who used atracurium and gallamine whereas, we employed pipecuronium; therefore discrepancies could be attributed to difference in the neuromuscular blocker employed. Roxatidine acetate, a new H 2 receptor antagonist with profound inhibition of gastric secretion[18] appears to reduce the risk of aspiration pneumonitis by decreasing the volume and increasing the pH.[19] In the present study, lower dose (0.05 mg/kg) did not produce any change in the contractile twitch response while intermediate (0.2 mg/kg) and higher dose (0.5 mg/kg) produced significant paralysis, which reached to steady state in 30 min. Bossa et al[11] reported similar observations; however, they used very high dose of roxatidine acetate (i.e. 40 and 80 mg/kg i.v.) in the preparation stimulated at high (3 Hz) frequency. In the present study, we used very low doses (i.e., 0.2 mg/kg and 0.5 mg/kg) of roxatidine acetate in the preparation stimulated at low (0.5 Hz) frequency, which may be relevant to the clinical situation. The mechanism by which roxatidine acetate significantly reduced the contractile twitch responses could be ascribed to an action at presynaptic level, mediated by decrease in calcium influx.[11] Lower dose (0.05 mg/kg), of roxatidine acetate did not alter pipecuronium-induced paralysis (ID 50 value), while it significantly increased the time required for the onset of paralysis without modifying the time required for to develop peak effect and recovery from the paralysis. While intermediate dose (0.2 mg/kg) roxatidine significantly antagonized pipecuronium-induced paralysis (increased in ID 50 value) and increased the time required for the onset of peak effect, without affecting the recovery time. Roxatidine acetate produced biphasic effects on the isolated rat phrenic nerve hemidiaphragm preparation.[20] This effect is similar to that produced by depolarising blockers, i.e., dual action with initial potentiation of the basal contractile twitch responses (agonistic action) at lower doses followed by blockade at higher doses. Similarly high dose of roxatidine acetate (40 mg/kg) potentiated the basal contractions in vivo .[11] However, in the present in vivo study such agonistic activity was not observed probably because lower dose of roxatidine acetate was employed. In the light of the above observations, antagonism of pipecuronium-induced paralysis could be attributed due to agonist action of roxatidine acetate.[11],[20] Also, increase in the time required for onset and peak paralysis could be explained on the basis of the above agonistic action. The time required for recovery from pipecuronium-induced paralysis was not significantly altered by either lower (0.05 mg/kg) or intermediate doses (0.2 mg/kg) of roxatidine acetate. Higher dose (0.5 mg/kg) of roxatidine acetate produced significant enhancement of pipecuronium-induced paralysis with significant increase in the time required to produce peak paralysis as well as recovery from the paralysis. Enhancement of d-tubocurarine,[11] pancuronium[21] and vecuronium[20] induced paralysis by roxatidine acetate has been reported. The mechanism of potentiation of pipecuronium-induced paralysis by roxatidine acetate could be due to decrease in calcium influx at presynaptic site.[11] However, Choksi[20] reported that in isolated rat phrenic nerve hemidiaphragm preparation the neuromuscular blockade produced by higher concentration of roxatidine acetate was not reversed by calcium chloride, neostigmine and potassium chloride suggesting a depolarising type of block of roxatidine acetate. It is reported that prior administration of a depolarising blocker antagonized or had no effect on the paralysis produced by non-depolarising neuromuscular blocker.[22] However, in the present study, higher dose (0.5 mg/kg) of roxatidine acetate enhanced the paralysis produced by pipecuronium. Hence, it could be presumed that the blockade by roxatidine acetate at neuromuscular junction could be due to desensitization of nicotinic receptor as reported for some drugs.[23] However, further work is required to delineate the exact mechanism of potentiation of pipecuronium-induced paralysis by higher dose of roxatidine acetate. Conclusion It is concluded that since famotidine per se had no effect on twitch responses and had produced less pharmacodynamic drug interaction as compared to roxatidine acetate with pipecuronium, it may be preferred as pre-medication agent in clinical practice. Besides roxatidine acetate blocked, the twitch responses of the gastrocnemius sciatic nerve preparation suggesting caution in its use especially in patients receiving drugs that depresses neuromuscular transmission e.g., aminoglycoside antibiotics. Hence, careful monitoring should be planned to prevent complications due to drug interactions with neuromuscular blockers. Also, decrease in dose of pipecuronium or other non-depolarizing agent is suggested when H 2 antagonists are used as preanaesthetic agents. Hence, these drugs should be administered with careful monitoring in such patients as vital functions may be affected.References
Copyright 2007 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph07004t2.jpg] [ph07004t3.jpg] [ph07004t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}