 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
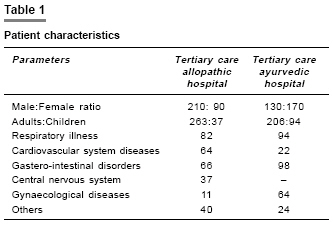
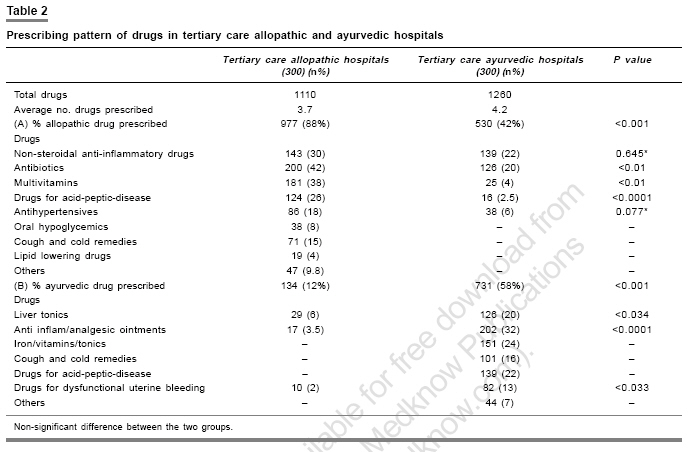
Indian Journal of Pharmacology, Vol. 39, No. 1, January-February, 2007, pp. 52-54 Research Letter Allopathic vs. ayurvedic practices in tertiary care institutes of urban North India Verma Ujala, Sharma Rashmi, Gupta Pankaj, Gupta Samta, Kapoor Bhuvneshvar Postgraduate Department of Pharmacology and Therapeutics, Govt. Medical College, Jammu Code Number: ph07012 The National Center for Complementary and Alternative Medicine (NCCAM) defines complementary and alternative medicine (CAM) practices as those not presently considered an integral part of conventional medicine.[1] Important aspects of Alternative medical systems include traditional oriental medicine, homeopathy and Ayurveda. Utilization of CAM is a universal phenomenon, both in developing countries as well as in developed countries like USA.[1],[2] Ayurveda, the oldest herbal system of medicine is the most commonly practiced form of CAM in India fulfilling the medical needs of 80% of the population.[3] However, the supreme court ruling forbids the doctors of modern medicine from prescribing/administration of non-allopathic drugs (such as Ayurvedic, Unani, Siddha or Homeopathic) by rendering them liable to prosecution under both civil and criminal laws leading to cancellation of registration and/or imprisonment. As such they are liable to be labeled as ′quacks′ per se without further evidence or argument.[4] Still the popularity of ayurvedic drugs among allopathic practitioners is on rise. Since, there is dearth of data regarding the use of allopathic and ayurvedic drugs by different practitioners, a pilot prospective study was undertaken to evaluate the prescribing pattern of allopathic and ayurvedic drugs in the medicine out patient department (OPD) of the tertiary care allopathic hospital (TCALH) and ayurvedic hospital (TCAYH) after taking consent from respective Institutional Review Boards during the period between August 2005 and November 2005. Both the hospitals belong to government setup. TCALH and TCAYH are situated 1.5 kms apart in the heart of the city. Two investigators each were allotted to follow the prescription study in TCALH and TCAYH. From each hospital 300 prescriptions were collected [Table - 1]. As the total number of patients attending TCALH (about 100 patients per day) were more in number as compared to those attending the TCAYH (about 60 patients per day), the investigators decided to evaluate every fifth prescription in the TCALH and every third prescription in the TCAYH. Each investigator visited the respective OPD on fixed days of the week and collected prescription slips after taking consent from the patient or attendant. After noting down the required parameters like nature of the drug used (Ayurvedic/Allopathic/class of drug), number of drugs per prescription, prescription slips were returned back to the patients. The percentage of various drugs used in both the hospitals was compared using Chi-square test. P -value < 0.001 was considered statistically significant. Average number of drugs prescribed was more in TCAYH (4.2) than TCALH (3.7). The prescriptions of TCALH contained 88% allopathic and 12% Ayurvedic drugs; on the other hand prescriptions of the allopathic drugs by the Ayurvedic practitioners was found to the tune of 58% ( P -value < 0.001) [Table - 2]. In the TCALH, NSAIDS (non-steroidal-anti-inflammatory drugs), antibiotics, multivitamins, drugs for acid-peptic-disease (APD) constituted the bulk of the allopathic drugs prescribed. Whereas, drugs like liver tonics, analgesic ointments and drugs for dysfunctional-uterine-bleeding were the main Ayurvedic drugs prescribed [Table - 2]. However, these Ayurvedic drugs are available as over the counter drugs in India. The ayurvedic practitioners were found to prescribe mainly ayurvedic drugs including liver tonics, anti-inflammatory and analgesic ointments, iron, vitamin tonics, drugs for cold and APD. However, the commonly prescribed allopathic drugs were NSAIDS (22%) and antibiotics (20%) [Table - 2]. In a previous study from India it was reported that ayurvedic drugs were prescribed by 5.26% of allopathic- practitioners; whereas, allopathic drugs such as anti-histaminics/cough syrups/decongestants, bronchodilators and steroids were prescribed by more than 80% of ayurvedic practitioners in the private setup.[5] Similarly, in a study from Sri-Lanka using trained ′pseudo-patients′ the prescribing of allopathic medicine by ayurvedic practitioners was reported.[6] However, our study has been conducted on the real patients, having genuine complaints who voluntarily chose their prescribers. The sample of our study is hospital-based and covers only the urban population and qualified practitioners, ignoring the millions of prescriptions from the registered medical practitioners and quacks practicing freely in remote corners of our country, which could be considered as llacuna of the present study. Other factors influencing the prescribing pattern of the prescribers like sex, qualification and age were also not recorded in the present study. The patients were not followed for interactions and side effects. The use of CAM in the general population around the world ranges from 9 to 65%.[7] However, less than 40% of the patients discuss their use of CAM therapies with their primary care physicians assuming that these products are inert or at least innocuous.[1] But contrary to the common belief, even the herbs used for thousands of years have the potential to cause adverse effects and interactions with other medications.[1] These adverse outcomes with the use of herbs may be due to the impurities, unnamed adulterants or batch-to-batch variability.[1] Since many alternative medicinal substances are legally considered dietary supplements, these do not come with in the preview of FDA (Food and Drug Administration). However, these are governed under Current Good Manufacturing practice in Manufacturing, Packaging or Holding Human Food (CGMP) regulations.[1] Moreover, according to Dietary Supplement and Health Education Act (DSHEA) passed by United States Congress in 1994, proof of safety or efficacy is not a prerequisite for the marketing of dietary supplements.[1] A draft law reminiscent of the Dietary Supplement Health and Education Act (DSHEA) is in development in India to regulate manufacturing, importing and marketing of health foods/dietary supplements and other nutraceuticals. The Indian Food Safety and Standards Bill 2005 has been signed into law, promising a significant impact on the Indian dietary supplement industry and encouraging manufacturers to do new product development, develop reliable testing protocols, carry out clinical studies and establish structure-function claims based on these studies.[8] The results of our study clearly indicated the popularity of cross-pathy practices among both qualified allopathic and ayurvedic practitioners. However, Clause1.1.3 of Medical Council of India (MCI) prohibit the allopathic practitioners to prescribe drugs from Ayurvedic System of Medicine and ayurvedic practitioners from Allopathic System of Medicine.[9] Hence, there is urgent need to undertake educational and reorientation programmes of registered medical practitioners regarding various MCI rules and regulations. Even the ayurvedic practitioners need to be adequately trained to recognize conditions that require referrals to the allopathic practitioners. Moreover, large scale epidemiological studies should be conducted both in the urban and rural parts of the country, comparing the trend of cross-pathy practices among qualified practitioners of both the systems of medicine; as well as comparing the trend of CAM and allopathic drugs use as self-medication between different sections of the society. Nonetheless, high quality, clinical trials are required to establish the safety and efficacy of ayurvedic drugs. The benefit of the patient lies in the optimal balance and evidence-based use of the two systems and this needs to be encouraged especially in developing countries like India with inadequate doctor patient ratio. References
Copyright 2007 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph07012t1.jpg] [ph07012t2.jpg] |
| |||||||||

{kind=link}
{kind=link}