 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
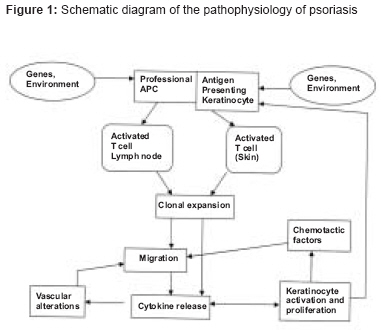
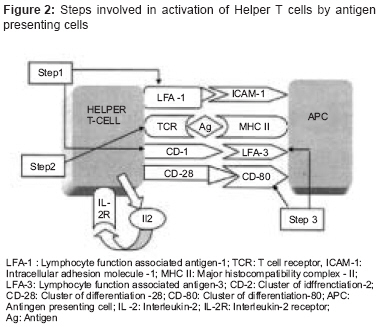
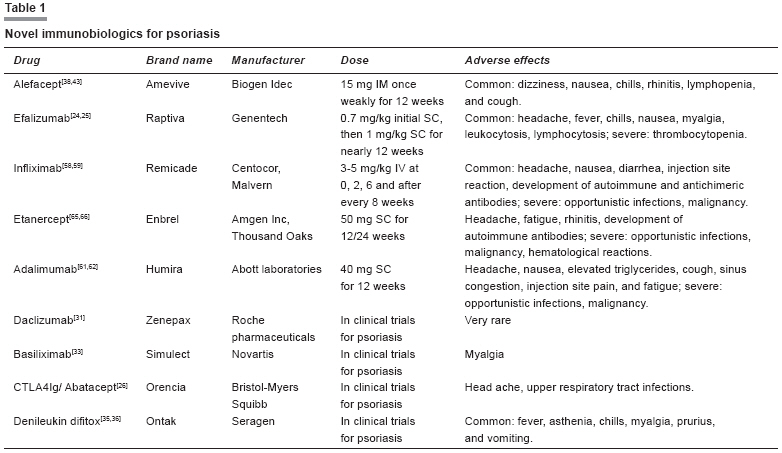
Indian Journal of Pharmacology, Vol. 40, No. 3, May-June, 2008, pp. 95-102 Review Article Novel immunobiologics for psoriasis Ghosh Nilanjan, Singh PN, Kumar Vikas Department of Pharmaceutics, Institute of Technology, Banaras Hindu University, Varanasi-221 005 Date of Submission: 24-Aug-2007 Code Number: ph08034 Abstract Psoriasis is one of the most common human skin diseases and is considered to have key genetic contributions. It is characterized by excessive growth and aberrant differentiation of keratinocytes, but is reversible with appropriate therapy with the possibilities of recurrence. The trigger of the keratinocyte response is thought to be the activation of the cellular immune system with T cells, dendritic cells and various immune related cytokines and chemokines being implicated in pathogenesis. Immunosuppressants like cyclosporine and methotrexate were used earlier in the treatment of psoriasis, however their use was associated with severe adverse effects due to down regulation of immune system. The most recent advances in therapies for psoriasis target specific immune components of psoriasis and promise to have high therapeutic efficacy with low adverse effects. This review focuses on the novel therapies aimed to specifically modulate the dysregulated immune system with minimal adverse effects.Keywords: Antigen presenting cells, cytokines, helper T cells, psoriasis Introduction Psoriasis is an immune mediated genetic papulosquamous skin disorder which affects approximately 3% of world population. A substantial proportion of patients with psoriasis may develop a form of inflammatory arthritis known as psoriatic arthritis which contributes significantly to patient′s disease burden with physical disability, pain and further reduction in quality of life. [1] Based on histological manifestation, in the past psoriasis was understood to be a disorder of keratinocyte hyper proliferation. However recently, with understanding of the etiology of the disease and the success of immunosuppressive therapies, the paradigm for understanding the disease has shifted towards T cell pathogenesis. Standard immunosuppressive therapies (like cyclosporine, methotrexate, hydroxyurea etc) which were used to treat psoriasis target different components of the immune response or block keratinocyte proliferation. However, these treatments are also associated with serious adverse effects like bone marrow depression, severe hepatotoxicity, renal dysfunction, gastrointestinal toxicity etc and may fail to induce long remission thus many patients elect not to undergo therapy. [2] In light of these pitfalls, much effort has been focused on immunobiologic agents, representing alternative approaches which are not only safe and effective but also allow longer remissions. Here we discuss the immunobiologics as novel therapeutic approaches for treatment of psoriasis. Types of psoriasis [3] Guttate psoriasis : It presents as small tear drop-shaped lesions on trunk and more proximal areas of extremities. Flexural psoriasis : When lesions affect major skin folds particularly in genital regions, armpits and under the breasts, it is said to be flexural psoriasis or also inverse psoriasis. Scaly nature of lesions is absent in this type. Pustular psoriasis : Patients with this type of psoriasis are often febrile with accompanying eruption of pustules over trunk and extremities. Psoriatic erythoderma : It is characterized by total involvement of skin by active psoriasis. [3] Genetics of psoriasis Pathogenesis of disease Langerhan Cell (LC) and Dendritic cell (DC) changes: The initial changes involve the immature dendritic cells (DC) and Langerhan cells (LC) in the epidermis, which capture and internalize the antigen. This is then processed and presented on the cell surface, bound to class I and II major histocompatibility complex molecules. In addition, the LC also acquires a number of cell surface receptor markers such as CD80, CD86, CD40, CD83, and intercellular adhesion molecule (ICAM) 1. This "mature" LC is now primed for stimulating the T cells in the draining lymph nodes. Subsequent T cell events lead to the activation of naive T cells in the lymph nodes into memory-effector (CD45RO) cells, differentiation and proliferation of these CD45 + cells. [9] Migration of activated T cells to sites of antigen excess in the skin, endothelial changes, expression of cell markers, and elaboration of various cytokines and adhesion molecules enhance this process and secretion of proinflammatory T1 cytokines by the effector T cells in the dermis and epidermis, with subsequent effects on keratinocyte proliferation. [10] The pathophysiology of psoriasis is shown in [Figure - 1]. T-cell activation is a multi step process which involves: Binding: Contact between the APC and the T cell is established by ICAM-1 and lymphocyte function-associated antigen (LFA) 3 on the APC with LFA-1 and CD2 on the T cells, respectively. Primary stimulation/signal 1: The primary event is the recognition of the major histocompatibility complex-bound antigen by an appropriate T-cell receptor. Once a match occurs, T cell gets activated, with increase in the synthesis of mRNA for IL-2 and IL-2 receptor (CD25). Thus, the primary signal is always antigen-specific. [10] Co stimulation/signal 2: Additional interactions also take place between the T cell and APC, together described as "accessory" or "co stimulatory signals". These are critical for optimal activation of the T lymphocyte. In the absence of co stimulation, the degree of responsiveness of the cell is very limited (anergy), or the cell itself may undergo apoptosis. These co stimulatory signals are not antigen-specific. Co stimulatory interactions include: (i) CD80 and CD86 on the APC with CD28 on T cell, (ii) CD80 and CD86 on the APC with cutaneous T-lymphocyte antigen (CTLA) 4 on the T cell, which is an inhibitory signal, (iii) LFA3 with CD2, and (iv) CD40 and CD40 L. IL-2 from T cells and IL-12 from mature LCs also bind to their receptors on the activated T cells. These reactions regulate transcription of cytokines such as interferon IFN-γ, TNF-α, IL-2, and granulocyte-macrophage colony-stimulating factor (GMCSF). These cytokines are responsible for differentiation, maturation, and proliferation (mitotic activity) of the T cells into memory-effector cells. The naive T cells are thus processed to mature into T H 1 and type 1 cytotoxic T cell producing type 1 cytokines. Some of the T cells may also differentiate toward natural killer cell formation, which react with nonprotein antigens. [11] The steps involved in activation of helper T cells by antigen presenting cells are depicted in [Figure - 2]. Efferent arm: The efferent arm includes the processes involved in migration of T cells to the site of antigen excess in the inflamed skin and their subsequent effects on keratinocytes. Migration of effector T cells to the site of antigen excess in the inflamed skin is the next step. T cells acquire a surface protein termed cutaneous lymphocyte-associated antigen. This is an adhesion molecule that mediates attachment of the T cell to the endothelial cells of the dermal vasculature (through E selectin and P selectin), with subsequent entry into the skin. The process also involves triggering of many chemokines and binding of integrins such as vascular cell adhesion molecule (VCAM), intercellular adhesion molecule (ICAM-1), and LFA-1. Effects of T cells on site: Once in the dermis, the T H 1 and type 1 cytotoxic T cells release high levels of IFN-γ and TNF-α. These induce ICAM-1, CD40, and major histocompatibility complex II proteins on the keratinocytes. Intraepidermal T cells trigger keratinocyte hyper proliferation, which accelerates epidermal growth occurring in the regenerative pathway. [12] It is likely that a cascade of cytokines, secreted by different cells in the local environment of the psoriatic plaque, play a role in the phenotypic responses in psoriasis. TNF-α has been found to increase type I vasoactive intestinal peptide (VIP) receptor mRNA in keratinocytes. Vasoactive intestinal peptide promotes keratinocyte proliferation and stimulates synthesis of proinflammatory cytokines such as IL-6, IL-8, and RANTES (regulated upon expression, normal T cell expressed and secreted). [13] These cytokines from intraepidermal T cells have been shown to be direct keratinocyte mitogens and thus could directly stimulate keratinocyte proliferation. TNF-α also increases plasminogen activator inhibitor type 2, a serine proteinase inhibitor, which is thought to protect cells from apoptosis. [14] The prevention of apoptosis by this or other mechanisms could lead to increased longevity of keratinocytes and consequently to a thickened epidermis. IFN-γ is also a trigger for epidermal hyperplasia when injected into skin. The other proposed mechanisms for keratinocyte hyperplasia include wound reparative phenomenon that is triggered by intercellular disruption caused by T-cell entry into the epidermis. Mitogenic cytokines and receptors on keratinocytes such as epidermal growth factor (EGF), insulin like growth factor 1 and keratinocyte growth factor pathways are implicated in regenerative hyperplasia, and these would be stimulated as part of a wound repair response. [15] The other features of a psoriatic lesion, such as vascular proliferation and neutrophil infiltration are also caused by the action of the other cytokines such as vascular endothelial growth factor and IL-8 from keratinocytes on endothelium and polymorphonuclear leukocyte recruitment. [16] Development of immunobiologics Evaluation of biologics Action of immunobiologics Anti-CD4 antibody: OKTcdr4a. The underlying strategy behind OKTcdr4a (ORTHOCLONE), a humanized antihuman CD4 IgG4 monoclonal antibody derived from the murine OKT4A, is to prevent the generation of signal 1 in CD4+ cells. [20],[21],[22] In one small open label study, six patients with severe chronic plaque psoriasis were administered a total of three 1 mg/kg/day OKTcdr4a IV infusions every other day. After 4 weeks, patients experienced a mean reduction of 46% from baseline PASI values. One patient did not respond to treatment. Of the five responders, disease remission lasted 6 months in three patients and up to 1 year in one patient. Signal 2 inhibition Anti-B7 antibodies: B7.1 (CD80) and B7.2 (CD86) are surface ligands APC′s which bind to T cell CD28 to provide co stimulatory signals, as well as CTLA4 (CD152) to inhibit further T cell activation. As an inhibitor of the immune response, CTLA4 is expressed only on activated T cells and possesses a higher binding affinity for B7 than CD28. CTLA4Ig/Abatacept IDEC-114 Targeting pathogenic T cells Anti-IL-2R Anti-CD25 antibodies Basiliximab IL-2 fusion toxins: DAB (389) IL-2 (Denileukin Diftitox) Anti-CD2 antibodies Alefacept none MEDI-507 Immune deviation Tenovil (rhIL-10) Oprelvekin (rhIL-11) rhuIL-4 Cytokine inhibitors Infliximab Adalimumab Etanercept Toxicity of immunobiologics Infections Neurological disease
Cardiovascular disease Antinuclear antibodies and lupus like syndrome Hepatitis Thrombocytopenia Conclusion We are at the dawn of a new era of effective immune modifying therapeutics for psoriasis. Although, efficacy of many of these agents is unquestionable, the longterm consequences of their immunomodulatory effect are yet to be firmly established. Responses may also vary between individuals, perhaps because of polymorphism in genes. With greater understanding of cutaneous immunology and further knowledge uncovering the mechanisms controlling the differentiation of activated T cells during an immune response, new biologic immune modifiers with highly specific immune targeted therapeutics can be developed that should have a better longterm safety than the currently available therapeutic agents.Acknowledgements We wish to thank Dr. D.K. Arulmozhi (Scientist, Advinus Therapeutics, Pune) for his critical comments on the manuscript References
Copyright 2008 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph08034f2.jpg] [ph08034t1.jpg] [ph08034f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}