 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Pharmacology, Vol. 41, No. 1, January-February, 2009, pp. 9-14 Research Article Comparison of safety, efficacy, and cost effectiveness of benzyl benzoate, permethrin, and ivermectin in patients of scabies Bachewar NarendraP, Thawani VijayR, Mali SmitaN, Gharpure KundaJ, Shingade VaishaliP, Dakhale GaneshN Government Medical College, Nagpur Date of Submission: 16-Oct-2008 Code Number: ph09003 Abstract Objective: To compare three treatment modalities in scabies for safety, efficacy, and economy in a local population of Nagpur.Materials and Methods: This was a prospective, randomized, comparative clinical trial conducted in 103 participants, randomly allocated to three groups. First group received benzyl benzoate (BB) 25% lotion, second group received permethrin 5% cream, whereas third group received tablet ivermectin 200 µg/kg as a single dose. The participants were recalled after one week for follow-up evaluation. If there were no signs of cure, the same intervention was repeated. The participants were followed up for two weeks for cure rate, adverse drug reaction (ADR) monitoring, and postintervention observation. The follow-up was stopped after two weeks. Statistics: Fischer's exact test using Graph pad Instat v 3.05. Results: Ivermectin showed 100% cure rate after two weeks of treatment. Permethrin decreased pruritus by 76% at the end of one week and had significantly better cure rate than ivermectin. At the end of two weeks treatment, this finding was reversed, that is, cure rate in ivermectin group was 100%. For cost-effectiveness analysis, treatment regimens were formulated hypothetically for comparison from Markov population tree for decision analysis. It was found that BB and ivermectin each consecutively for two weeks were most cost effective regimens giving complete cure in four weeks, while ivermectin was the fastest regimen giving the same results in two weeks. Conclusion: Benzyl benzoate as first line intervention and ivermectin in the remaining gave best cost-effective results in the study patients of scabies. Keywords: Efficacy, economic analysis, scabies, treatment Introduction The annual incidence of scabies being three million, the disease burden on the developing countries justifies this study [1],[2] in India. Scabies is of greater importance due to its affinity for economically marginalized and immunocompromised hosts. [3] Sarcoptes scabie gains its importance by making the host morbid by its lesions, immense pruritus, high infectivity, frequent relapses, persistence of symptoms for many days even after eradication, and resistance to the routine treatment. [4] Treatment of scabies has changed from Celsus to modern medicine, from sulfur to permethrin and ivermectin. [5] Current treatment of scabies comprises of topical antiscabetics, applied all over the body for a specified contact period. [1] Research has been attempted to find the best antiscabetic focusing on efficacy and safety data. [6] Indian population being commonly affected by scabies, masses have poor affordability for the most efficacious antiscabetic. Hence, it was decided to study and compare three antiscabetics - the most commonly used benzyl benzoate, the currently considered medicine of choice permethrin, and the most recently introduced ivermectin - in the local population of Nagpur. Aim Objectives
Materials and Methods Study design Patients willing to participate were screened by applying the inclusion and exclusion criteria. Inclusion criteria included newly diagnosed patients of scabies, of either gender, above 12 years of age, willing to participate, and give written informed consent. For inclusion, the patients had to satisfy at least three out of the five criteria viz. history of contact with a scabies patient, complaint of nocturnal itching, history of involvement of family members, presence of classical burrows on clinical examination, and presence of typical scabetic lesions like papules, nodules, or vesicles. Exclusion criteria included pregnant or lactating women; women of child bearing age or planning for conception in near future; participants with abnormal liver and kidney functions, known thyroid disease, cardiac disorders, nervous system disorders, and psychiatric illnesses; and participants with history of diabetes mellitus, hypertension, or chronic infectious diseases. Participants taking any concurrent medication for other illness, consuming tobacco in any form, alcohol, or any substance of abuse were excluded from the trial. Participants with any other associated skin disease, which could alter the picture of scabies; known/suspected immunocompromised individuals, having scabies with atypical presentations like crusted scabies or scabies incognito; participants who had taken any antiscabetic treatment in the preceding week; and noncompliant participants were excluded. In this trial ivermectin was given as supervised [7] medication along with printed handouts of "do′s" in the local vernacular language. During their second visit, those participants who failed to answer correctly the method of application followed by them and the treatment of fomite were considered as noncompliant. Participants were first treated for the secondary infection, if present, with azithromycin 500 mg once daily for three days/ampicillin 500 mg 6 hourly for five days, as per clinical judgment of the senior dermatologist and subsequently included in the trial. The demographic data of the participants like age, gender, occupation, education, and marital status were collected in the case record form (CRF) by the principle investigator (PI). At each visit the participant was examined by two doctors, a dermatologist and the PI. The 103 enrolled participants were allocated to three groups according to random allocation number generated through computer and provided with any one of the chosen three therapeutic interventions. Participants were advised not to use or mix any other treatment, including antipruritic or antihistaminic medicines. All participants were issued 25% benzyl benzoate (BB) lotion for topical application for the family members and close contacts, as per the standard treatment guidelines to check the reinfestation of the trial participants. Participants were reinforced with the message about treatment of the family members and other close contacts during each visit. Interventions
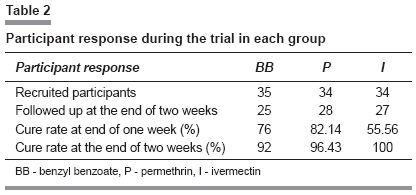
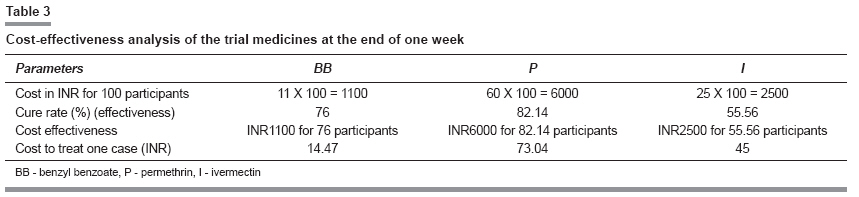
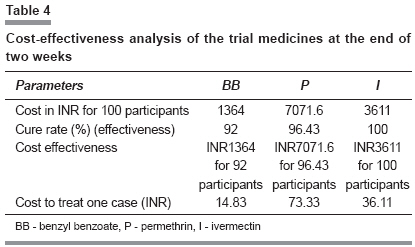
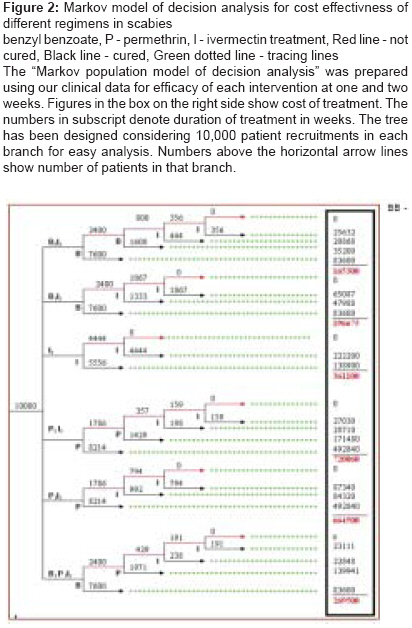
Participants on intervention I and II were advised to bathe with warm water before application of medication and on subsequent morning. The participants were recalled after one week for follow-up evaluation. The same intervention was repeated if there were no signs of improvement. The participants were followed up for two weeks for cure rate, adverse drug reaction (ADR) monitoring, and postintervention observation. Because of the known safety of all the three interventions, no laboratory examinations were advised. The follow-up was stopped after two weeks subject to achievement of one of the three endpoints - participant defined as completely cured, participant who developed severe ADR, or participant who was not cured two weeks postintervention follow up. Cure Pruritus Statistical analysis Results While doing randomized sampling for this study, gender-wise distribution and the follow-up in all the three treatment groups was maintained throughout the trial, except the BB group in which we experienced lower follow up in women. The same ratios as in followed-up groups were maintained in cure rates at the end of two weeks [Table - 1]. Living status - living singly or with a partner - did not show any implication over cure rates with any of the treatments. Majority (84%) of the participants were from 12-41 years age group, showing the usual trend of scabies. [6] Most (85%) of the participants had at least primary education. This confirms their literacy and ability to understand the written instructions provided to them. The distribution of typical scabies lesions over different body parts was variable. To enumerate the important ones, pubic region lead with 18%, followed by abdomen, wrists, and web space affliction amounting 13% each, and cubital region was affected in 11%. Ivermectin was least promising at the end of one-week treatment, but it showed 100% cure rate after two-week treatment [Table - 2]. Considering pruritus as presenting symptom, the medication which alleviates it has greater acceptance in clinical practice. We observed that permethrin qualifies for this, with 76% decrease in pruritus at the end of one week. Statistical analysis with Fisher′s exact test showed that at the end of one week, considering the cure rate, only permethrin was significantly ( P < 0.05) better than ivermectin. At the end of two-week treatment, this finding was reversed because the cure rate in ivermectin group was 100%. Economic analysis Cost effective analysis Cost-effectiveness graph Incremental cost = cost of the new (second) treatment - cost of the old (first) treatment Incremental effectiveness = efficacy of new (second) treatment - efficacy of old (first) treatment Considering the cure rates at the end of one week, cost incurred to treat 100 participants for different interventions was found to be: Total cost of treatment = INR for participants cured with one week treatment + INR for participants who were treated for two weeks Cost of one bottle of BB was INR11, for one permethrin tube was INR60, and that of one 12 mg tablet of ivermectin was INR25. With these costs the cost of treatment in INR was calculated as: Benzyl benzoate = (11 X 76) + (22 X 24) = 1364 Amount needed to treat one case of scabies successfully at the end of one week was least for BB with INR14.47 and it was most for permethrin with INR73.04 [Table - 3]. All the values thus obtained were used for further analysis. The same parameter at the end of two weeks was again least for BB with INR14.83 and was most for permethrin with INR73.33. Thus, permethrin was approximately five times costlier for treating one scabies case successfully at the end of one- or two-week treatment [Table - 4] The cost-effectiveness graphs confirm that as compared to permethrin, BB and ivermectin fall in acceptability zone. Ivermectin falls at the center of acceptability zone, thereby suggesting that it is more cost effective than BB [Figure - 1]. Markov model of decision analysis [8],[9] In this trial the cure rate of ivermectin was found to be 100% at the end of two-week treatment. We formulated various regimens after permutations and combinations to gain 100% cure rate for the treatment of scabies patients in the tertiary care institution level. We formulated the regimens considering the cure rates of all the three medicines of this trial, which we got at the end of one- and two-week treatment. The hypothetical regimens were:
where subscript denotes the number of weeks for which the treatment is given. The alphabets denote the medicine given for that duration, for example, B 2 I 2 means benzyl benzoate treatment given for two weeks and then uncured patients treated with ivermectin treatment for next two weeks. Among all the regimens, ivermectin had the shortest duration of two weeks. All the regimens have two-week treatment with ivermectin at the end because in this trial we found ivermectin having 100% cure rate at the end of two weeks. None of the other two medicines offered such a cure rate. Markov population model of decision analysis shows that B 2 I 2 is the cheapest regimen, while I 2 gives the fastest results in half the duration with double the cost of B 2 I 2 . The third one which falls in between is, B 1 I 2, also a cost-effective regimen giving 100% cure in three weeks. Discussion Cure rates Economic studies Safety Finding the best option Ivermectin is the future drug of choice for scabies. [5] In France ivermectin is licensed for human scabies since 2001. [24] The treatment is easy, quick, safe, and well tolerated with maximal patient compliance. [24] Our findings show that BB required the least INR to treat one case of scabies, ivermectin was the most cost effective single medicine by virtue of its 100% efficacy, and permethrin gave the fastest symptomatic relief. After these confounding findings, we tried various permutations and combinations of regimes to obtain optimum desirable results, which added to the novelty of this research. Safetywise, we found the three medicines equal as no ADR was reported with any of these. Thus, only the cost effectiveness played the decisive role in selection. On Markov tree for decision analysis, [8],[9] we found BB as the preferred medicine. Our finding of B 2 I 2 as the most economical regimen recommends that one should start with BB treatment for scabies afflicted for first two weeks and then shift the uncured patients to oral ivermectin therapy for next two weeks. In another study where oral ivermectin was comapred to topical 10% BB, it was found that absolute results favored the use of ivermectin, but the difference was not statistically significant. [20] A recent trial proved that ivermectin significantly decreased post-treatment reinfestation as compared to permethrin, but the cause remained obscure. [25] On the basis of such results many researchers, regulatory bodies, and WHO recommend ivermectin use for mass treatment of scabies. [26] Ivermectin cannot be the best drug in every hospital setting; in spite of showing promise in its efficacy and safety, as the local resistance pattern (which we did not find) and the affordability of patient population varies, and other cheaper alternatives still have an important role in marginalized economies. We agree that addition of ivermectin to the clinician′s armamentarium should be welcomed for the treatment of scabies, as it is the most cost effective, safe medicine which gives relief in the shortest possible time. [22] Currently, permethrin is commonly recommended as the drug of choice. But in our study it did not get that coveted position. If we evaluate the best symptomatic treatment which can give moderate cure rate, permethrin is the answer. It is also equally safe. However, we did not find it in our recommendation because of the usual practice of giving additional antipruritic along with antiscabetics right at the very first visit for symptomatic benefit to all patients. Additionally, the result of highest cure rate with permethrin, which we found at the end of one week, did not sustain after two weeks. Limitations Conclusion In Government hospital like ours, we recommend that each patient of scabies should be first advised BB topically for two weeks. Nonresponders should then be advised oral ivermectin once a week for two weeks. In case of affording patients ivermectin once a week for two weeks currently offers quick, better, and safe results, restricting further morbidity and secondary transmission. The novel research design of clinical trial with economic analysis is easy and accurate method for doing a pragmatic trial, which can be replicated in other diseases.Acknowledgments We are indebted to the staff of Department of Skin and VD, headed by Dr. R.P Singh, Dr. Rathi, Dr. Riaz, Dr. Shyamal, Dr. Kirti, and Dr. Piyush. We also thank all the participants of this clinical trial. References
Copyright 2009 - Indian Journal of Pharmacology The following images related to this document are available:Photo images[ph09003f1.jpg] [ph09003t1.jpg] [ph09003t3.jpg] [ph09003t2.jpg] [ph09003f2.jpg] [ph09003t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}