 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Plastic Surgery, Vol. 36, No. 1, Jan-June, 2003, pp. 26-29 Preparation of Plaster Moulage (Cast) in Plastic Surgery patients Roshani E. Rana, Vinita A. Puri, Purnima M. Aiyer, Amresh Baliarsing Department of Plastic, Reconstructive Surgery and Burns, Seth G. S. Medical
College and K. E. M. Hospital, Parel,
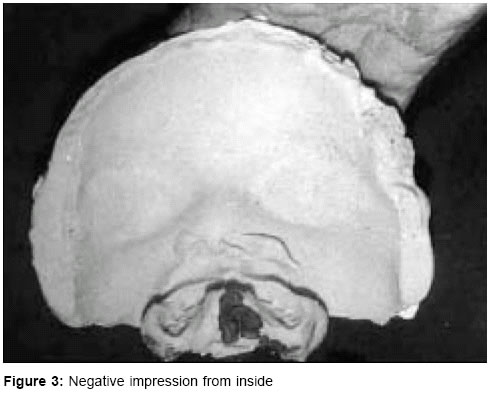
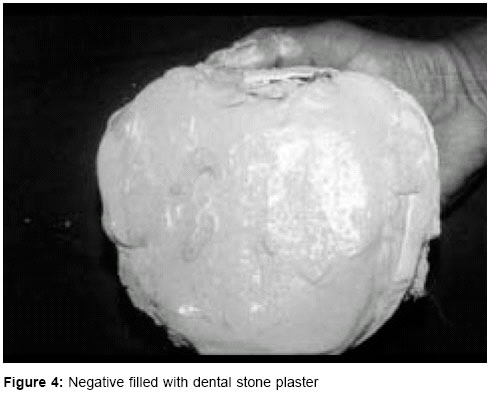
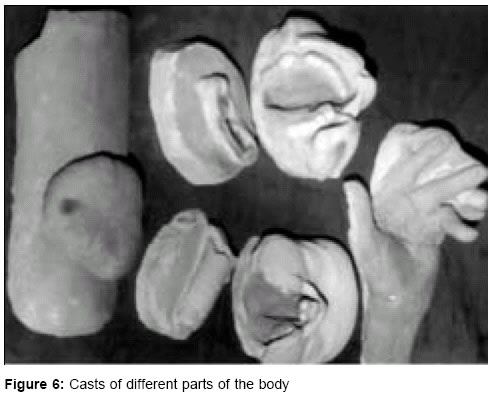
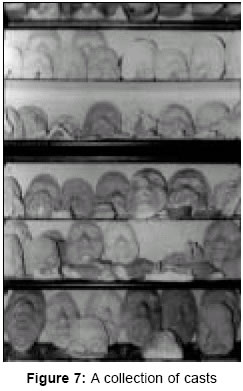
Mumbai-400012. Code Number: pl03006 ABSTRACT The purpose of this paper is to describe the technique of making casts using alginate compound for negative and dental stone plaster for positive impressions. With certain modifications a cast could be made of any part of the body and one can make a museum of interesting cases. Casts serve as useful teaching material especially in cleft lip and palate patients to study the effect of surgery on growth and development of the cleft lip-palate-nose complex in relation to the remaining face. It also helps in planning reconstruction in cases of facial defects, recording serial changes in multistage surgery, pre-operative and post-operative comparison as in rhinoplasty, ear reconstruction, hand etc; for comparing results before and after treatment in keloid and hypertrophic scars, fabrication of implants and preparation of prosthesis. In spite of newer modalities like 3-D imaging and stereolithography, the usefulness of this old technique in certain interesting cases can not be denied. Key Words: Moulage, Facial moulage, Hand moulage, Cast of cleft lip and palate. INTRODUCTION For a plastic surgeon, detailed pre-operative record of a patient is very important for assessing post-operative results. In addition to clinical notes, radiographs, photographs and newer modalilties like 3-D computer graphics and stereolithography, a plaster cast model serves as a useful mode of study, record and teaching. It helps in planning reconstruction in facial defects, pre- and post-operative comparison as in cleft lip and palate, rhinoplasty, ear reconstruction, results before and after treatment on keloid and hypertrophic scars, fabrication of implants and preparation of prosthesis. Various materials have been used to make negative and positive impressions. During World War I, Kazanjian used plaster of paris for making both negative and positive impressions in war victims with facial injuries. Later, Brown and McDowell1 popularised the method for Rhinoplasty patients. Clarke2 described the use of wax, plaster of paris, rubber, agar and alginate material for making a negative mould; and wax or plaster of paris for a positive cast. Thompson et al 3 used silastic to make negative impression. We have followed C.V. -Mehendale's technique using alginate for negative and dental stone plaster for positive impression. To make a composite impression of the face with lip and palate is slightly difficult. An impression-taking palate-plate was moulded and individually made from dental impression material. Shatkin and Stark4 made composite impression in cleft lip and palate patients using wax for palatal impression tray. To prevent overflowing of the alginate, we have devised a metal template as described by Lamont.5 MATERIAL AND METHODS Modified Lamont template, Zelgan (Alginate impression material), dental stone plaster or plaster of paris powder, plaster of paris (POP) bandage, dental stent (dental impression material), rubber bowl and spatula, 2 steel bowls - one containing hot water and other cold, No.11 scalpel blade, tongue depressor, scissors, forceps, glass plate 1'x1', spirit lamp, vaseline, gauze pieces, micropore tape 1" Combined Cast of Face with Alveolus and Palate - in Cleft Lip and Palate Patients This is made just prior to surgery. No patient is given anaesthesia just to make a cast. Making of a cast, with practice and organization adds only 15-20 minutes to the anaesthesia time. One cast by itself is useful and interesting, but when another is made at the time of repair of palate and yet another if a secondary procedure is done, makes an interesting series. This gives a permanent record of growth and development of the cleft lip-palate-nose complex in relation to the remaining face. After securing the endotracheal tube, the throat is packed with two packs. A deep one around the endotracheal tube and a superficial one in the oral cavity. Position is given as for a cleft lip and palate surgery. The eyelids are covered with micropore tape. Vaseline is smeared over the face especially over the eyebrows so that separation of negative becomes easy. Modified Lamont's template is positioned around the head. A palate plate is made out of dental stent after moulding it over the alveolus and palate (Figure 1). It has an extension, which reaches out of the mouth and is bent outside. It is individually made and is perforated with a no. 11 scalpel blade or a drill to give a grip to the negative impression in Zelgan. The Zelgan (alginate) is mixed with water in a rubber bowl with a metal spatula in the proportion as recommended. Mixing has to be done quickly because the setting time of Zelgan is 3-5 minutes. The palatal plate is filled with Zelgan and applied over the alveolus and palate. Rest of the Zelgan is then applied over the face taking care that the nostrils, alveolar gap and alveolar sulcus are filled, avoiding air bubbles (Figure 2). When Zelgan has partially set, about 3-4 layers of strips of plaster of paris (POP) bandage are applied over it including the outer extension of the stent plate so that the POP bandage and the stent create a rigid form. This rigid form gives the correct relationship of the outer surface of the face and lips to the alveolus and avoids any distortion. The Lamont's plate is removed. Once the Zelgan and POP bandage are fully set, the whole mass of Zelgan, POP casing and palate plate are gently eased out in a downward and forward direction. Any broken pieces of Zelgan are looked for in the palate and oral cavity and removed. The superficial throat pack usually comes off with the negative cast. After thorough cleaning of the nose and throat, the deep pack is removed. Figure 3 shows the negative impression. The next step is to make a positive, which can be done while the assistant is preparing and draping the face or one can wrap the negative in a wet cloth and make the positive at the end of surgery. A thin paste of Dental stone plaster is slowly poured in the negative, gently tapping the POP casing while it is being poured to avoid air bubbles. Over this, a thick paste is poured to fill the whole mould (Figure 4). The cast is then inverted over a glass plate and allowed to dry. After about 2-3 hours, the POP casing and Zelgan are then gently peeled off in layers to expose the positive cast (Figure 5). The stent can be removed by warming over a spirit lamp. Date and identification are carved on the back of the cast. The cast can be painted to make it more attractive and highlight its features. Preparation of a face cast (without anaesthesia) Can be made in supine or sitting position. The procedure is explained to the patient. Lamont's template is positioned around the head. Micropore strips are applied over the eyelids. Vaseline is smeared over the face especially over the eyebrows to help separation of the mould. The patient is made to hold a metal airway between the teeth to facilitate breathing throughout the procedure. A gauze pack around the airway ensures that the impression material does not enter the mouth. The nostrils are packed with small gauze pieces, which are placed slightly inside the vestibule so that nostril margins are free. After ensuring that the patient is comfortable, one proceeds to make the negative and positive impressions as described before. The basic technique of making negative and positive being same, with certain modifications, a cast could be made of any part of the body (Figures 6 & 7). Preparation of a moulage of hand Hand is smeared with vaseline. A trough made of POP bandage (individually made) is filled with Zelgan and the hand is placed in it with palm facing downwards. Some more Zelgan is poured to cover the exposed parts of the dorsum of hand. When the Zelgan has partially set, strips of POP bandage are applied over it. Once the Zelgan and POP casing are dry, the hand is gently eased out from the negative. Stone plaster is poured in the negative and allowed to dry. After it is completely dry the POP casing and Zelgan are peeled off to expose the Positive. DISCUSSION A cast gives an undistorted 3-dimentional view and reproduces an object in form and surface texture identical in appearance with the original. Fine folds in mucosa, or fingertip ridges are recorded precisely with greater clarity than in a photographic print. Photographs do not give 3-dimentional view and tend to fade with time. Newer modalities like 3-D computer graphics6 and stereolithography7 for facial reconstruction may not be available to all and are prohibitively expensive. Although making a cast is slightly time-consuming, requires patience and practice in preparation, its usefulness is worth the effort made. A combined cast of face with alveolus and palate is useful to study the effect of lip repair on the maxillary arches in a unilateral cleft lip and palate; and on premaxilla in bilateral cleft lip and palate. An ordinary dental impression will show the arches but it will not give any idea regarding their relationship to the soft tissues and naso-maxillary complex. The technique is old, but one can use it to make a museum of interesting cases. The only disadvantages are that they need more storage space and can break. ACKNOWLEDGEMENT We wish to acknowledge Dr. C. V. Mehendale who had mastered this technique and trained the first author. REFERENCES
Copyright 2003 - Indian Journal of Plastic Surgery. The following images related to this document are available:Photo images[pl03006f7.jpg] [pl03006f4.jpg] [pl03006f3.jpg] [pl03006f5.jpg] [pl03006f6.jpg] [pl03006f2.jpg] [pl03006f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}