 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Plastic Surgery, Vol. 36, No. 1, Jan-June, 2003, pp. 36-38 Case Report Congenital proximal radioulnar synostosis B. B. Dogra, Manmohan Singh, Anil Malik Command Hospital (Southern Command) Pune-411040.
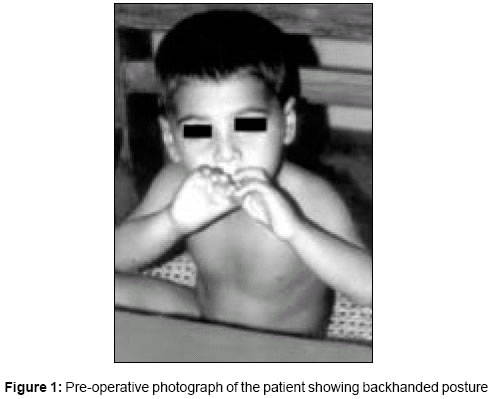
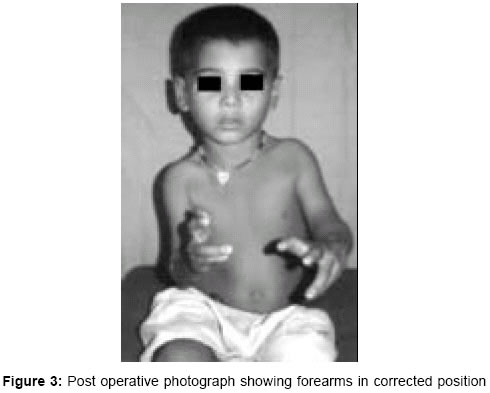
Code Number: pl03008 ABSTRACT Congenital proximal radio-ulnar synostosis is a rare anomaly and is often part of syndromes such as Crouzon, Apert's and Poland's. We have successfully managed one such case with bilateral involvement not associated with any other congenital deformity. He has been managed by performing derotation osteotomy through the synostosis mass with gratifying results. Key Words: Congenital, Radio-ulnar synostosis. INTRODUCTION Proximal Radio-ulnar Synostosis is a rare congenital anomaly, however it occurs more commonly than perceived and is often part of syndromes such as Crouzon, Apert's and Poland's. Although the exact etiology is not clear, but it has been documented that there is genetic basis for the failure of differentiation between the radius and ulna. During embryologic period the forearm is in pronation and the same position is found in almost all radio-ulnar synostosis.1 Proximal one third of forearm is the most common site of involvement, with male predilection. Patients generally present around the age of 3 years with functional problems such as difficulty in holding objects with both hands and in dressing and feeding themselves. Patients are usually seen holding objects with a backhanded posture. We present one such case of Congenital Proximal Radio-ulnar Synostosis, who has been successfully managed in this centre. CASE REPORT 4-years-old male child, born after 30 years of non-consanguineous marriage was brought with complaints of congenital absence of thumb in both hands, inability to rotate forearms, and holding of objects with back handed posture. There was no history of drug intake or viral fever during pregnancy. On examination, he was an active child with normal intelligence seen holding objects with back handed posture and griping the objects between index and middle finger (Figure 1). Local examination revealed that both forearms were in fixed full pronation and the wrist joints were radially deviated. The thumb was absent in both hands and there was duplication of index finger (left) and middle finger on right side. No other congenital anomalies were detected either clinically or radio logically. X ray both elbow joints revealed proximal osseous radio ulnar synostosis with diminutive radial head (Figure 2). Child was planned for a corrective derotation osteotomy on both sides in stages. A longitudinal dorsal incision was made over the u1nar ridge, extending from a fingerbreadth distal to the olecranon tip distally for about six cms. Sub-periosteal exposure of the fusion mass was accomplished. Transverse K wire was introduced through the synostosis mass over its distal end and derotation osteotomy carried out just proximal to this site. Axial K wire was passed from olecranon through the osteotomy site into the distal ulna. Using transverse K wire 60 degree de-rotation achieved, keeping the vascularity of the limb under check. Check X-ray taken after 6 weeks revealed satisfactory callous formation at the osteotomy site. He was taken up for similar procedure on the left side 06 months later and neutral position of forearm was achieved on this side. (Figure 3). DISCUSSION Radio-ulnar synostosis is regarded as an anomaly of longitudinal segmentation. It is presumed that some factor inhibits the interzonal mesenchyme between the cartilage analog of the developing radius and ulna from undergoing dissolution during the seventh week of intrauterine life. Thus, the interzonal mesenchyme persists and undergoes chondrification, ossification, and eventually synostosis. The proximal one-third of the forearm is the most common site of involvement. About 40 per cent of the cases are unilateral, and 60 percent bilateral. Males are affected more commonly than females. These children usually present with functional problems like difficulty in holding objects, two-handed posture and problems in dressing or feeding. They are often seen holding objects such as coins with a backhanded posture.2 Our patient is 4 year old male, with bilateral involvement, holding objects with a backhanded posture. Approximately one-third of patients with radio-ulnar synostosis have associated anomalies involving the cardiovascular, genitourinary, gastrointestinal, central nervous, and musculoskeletal systems.3 Our patient has none. Many have hand duplication or absence of digit3; our patient has absence of thumb of both hands, duplication of index finger in left and middle finger in right hand. Wilkie and Davenport in 1914 had described two types of synostosis based on radiographic appearance.1 Type 1 represents true radio-ulnar synostosis in which the radius and ulna are smoothly fused at their proximal ends and this extends for a variable distance distally. Type 2 is represented by congenital dislocation of head of radius in addition to type 1 deformity. Our patient has Type-I deformity. Cleary et al in 1985[4] observed four distinct patterns of radio-ulnar synostosis radiologically. Type I : Synostosis does not involve bone and
is associated with a reduced but normal appearing radial head.
Our patient had Type II radio-ulnar synostosis as per Cleary's classification. Patient with unilateral or bilateral deformities with less than 30 degrees of pronation generally do not require surgery. With more than 60 degrees or more of fixed pronation, there is obvious functional impairment in children with both unilateral and bilateral radio-ulnar synostosis.5 For those with between 30 and 60 degree of pronation, one must carefully individualize functional limitation and esthetic needs. Our patient had fixed pronation bilaterally. Various surgical options have been proposed to restore the correct position and mobility. These include resection of synostosis,1 insertion of swivel apparatuses, reconstruction with interpositional materials,6 rotational osteotomy through or distal to synostosis mass.4 Resection of synostosis, insertion of swivel apparatuses, reconstruction with interpositional materials, have been inconsistent over time because of bone overgrowth around implant materials and angulation of the forearm distal to the osteotomy therefore these procedure are of historical interest only. Derotational osteotomy through the area of synostosis is the functionally satistactory procedure and very popular.4,7 It preserves good cooptation of the divided ends and the osteotomy heals rapidly. As a great deal of rotatory correction is involved in the operation, the circulation must be carefully observed and undue stress during the correction should be avoided. The rotation should be performed in two stages if the correction to be obtained is significant, with a one to two week interval after surgery before further rotation is attempted.4 In our patient, we have performed derotational osteotomy through the area of synostosis and achieved 60-degree derotation on right side and mid prone position on left side. Fuminori Kanaya from Okinawa, Japan has recently come up with a very attractive method for mobilization of congenital proximal radio-ulnar synostosis using interpositional free vascularised fascio-fat graft. They harvested a fascio fat flap with a small monitoring skin island from the ipsilateral upper arm. The recurrent radial vessels were anastomosed to profunda brachii artery and vein. They have performed this procedure in seven boys with no resynostosis on follow up examinations 2 to 4 years postoperatively.8 The advantages of the technique we have employed in our case lie in the simplicity of the procedure, micro vascular anastomosis is not required hence it can also be carried out in a centre where such facilities are not available. REFERENCES
Copyright 2003 - Indian Journal of Plastic Surgery. The following images related to this document are available:Photo images[pl03008f2.gif] [pl03008f1.jpg] [pl03008f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}