 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
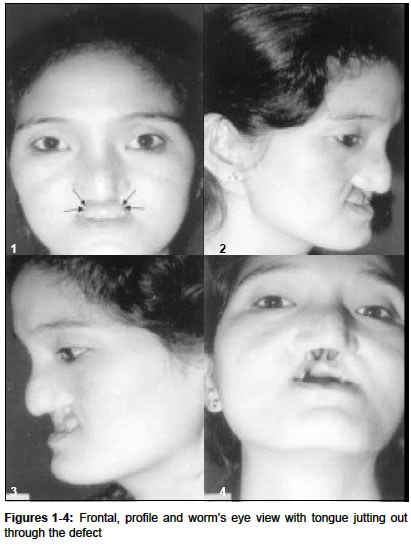
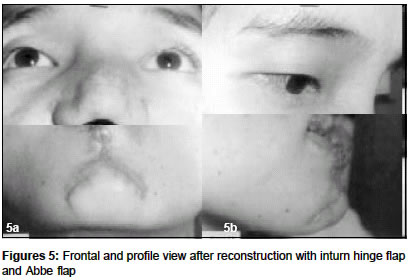
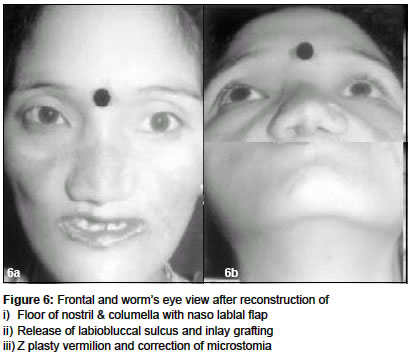
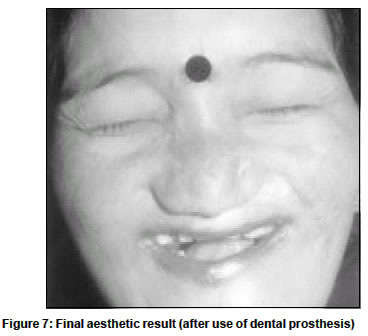
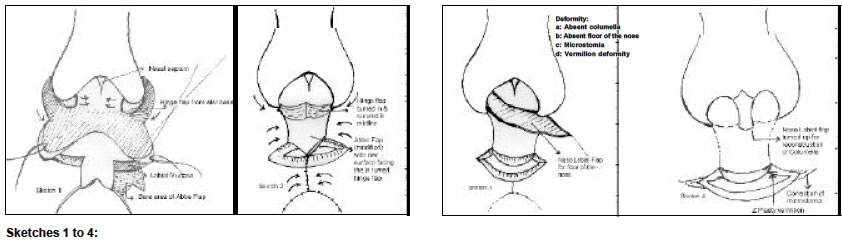
Indian Journal of Plastic Surgery, Vol. 36, No. 2, Dec, 2003, pp. 131-133 Case Report Aesthetic restoration of facial defect caused by cancrum oris: A case report Devi SR, Gogoi M Department of Plastic Surgery, Gauhati Medical College, Guwahati, Assam Code Number: pl03029 ABSTRACT A case report of cancrum oris deformity in a young lady with successful aesthetic restoration of defects is presented.INTRODUCTION Cancrum Oris (Noma) is a devastating infectious disease, which destroys the soft and hard tissues of the oral and para oral structures. However, it is very rare now, even in developing countries. It predominantly affects children between 2-16 years and is known to occur in association with poor nutrition and exanthematous infection. The chronic sequelae of the acute disease process leaves behind extensive deformities and often requires reconstructive surgery. The presentation of the disease is variable for the condition may affect the soft tissues of the face or the bones of the facial skeleton or both concurrently. It has a high mortality rate but with the introduction of antibiotics as a form of therapy, a higher survival rate has been achieved. As each case presentation is different it needs proper evaluation and careful treatment planning. The complex type of deformity usually requires staged reconstructive procedures. We are presenting a case report of a young lady with cancrum oris deformity with successful and aesthetic restoration of her defect CASE REPORT A 26-year-old girl presented with loss of 3/4th of the upper lip, anterior palate, membranous septum and columella with the tongue jutting out through her defect. She belonged to a poor socioeconomic group of Arunachal Pradesh and gave history of some infection in her face in her early childhood. The wound finally healed over a period of months leaving behind the grotesque deformity. [Figure - 1], [Figure - 2], [Figure - 3] & [Figure - 4] After careful evaluation of her defect and treatment planning we decided for staged reconstruction and explained this to the patient. In the first step, the upper lip remnant on both sides was released and an in-turn hinge flap was planned which was to form the base of the Abbe flap for support. The Abbe flap was modified keeping part of its mucosal surface bare so as to lie against the raw surface of the hinge flap. [Figure - 1] & [Figure - 2] In the second and third stages, a nasolabial flap from the left side was used for the reconstruction of the nostril sill and floor and finally it was turned upwards to form the anterior septum and the columella. Six months later, the labio buccal sulcus was released and an inlay skin graft was done. The patient was discharged with a dental mould compound kept in situ as a spacer. In the next stage, correction of microstomia and Z plasty of the vermilion border was done to maintain symmetry of the vermilion [Figure - 3], [Figure - 4], [Figure - 5] & [Figure:6] Finally a prosthesis with an obturator with central and lateral incisor was given for the anterior defect in the palate. Final Aesthetic result is shown. [Figure:7] DISCUSSION Cancrum oris is an infectious disease, which destroys the orofacial tissues and other neighbouring structures in its fulminating course. The exact bacteriology is uncertain although Vincent′s spirochaete and the fusiform bacillus in symbiosis have been considered to be the actual cause of the condition.[1] Because of the nature of the condition the morbidity rate is exceptionally high with functional disturbances and disfigurement being a legacy of the disease. Reconstructive procedures are generally required at some subsequent stage. The surgical treatment of the sequelae in the patients affected by cancrum oris (Noma) is possible if the surgeon carefully evaluates each patient individually choosing simple, safe, sound and satisfactory techniques, which are conditioned by sex and age of the patients.[2] The disease usually affects children aged 2-16 years particularly in Sub- Saharan Africa from 1-7 cases per 1000 population. Acute necrotizing gingivitis (ANG) and oral herpetic ulcers are considered to be the antecedent lesions, and infection with Fusobacterium necrophorum (Fn) and Prevotella intermedia (Pi) are the suspected key players. Additional to production of a growth- stimulating factor for Pi, Fn displays a classic endotoxin, a dermonecrotic toxin, a cytoplasmic toxin, and a haemolysin. Without appropriate treatment the mortality rate from Noma is 70-90%.[3] Nutritional deficiency is said to be one of the causative factors. In a study of Nigerian children[4] significantly reduced plasma concentration of Zinc (< 10.8 micro mol/L) retinol (< 1.05 micro mol/L), ascorbate (< 11 micro mol/L), and the essential amino acids, with prominently increased plasma and saliva levels of free cortisol, compared with their healthy counterparts was documented. Most of the strains of F necrophorum and P intermedia were found to be sensitive to clindamycin, metronidazole and penicillin except one strain of P intermedia, which showed resistance to penicillin.[5] There have been reports of one stage reconstruction of defects caused by Noma, which is both cost effective and safe.[6] However, in our case, we used staged procedures, which was well accepted by our patient. Except for two procedures, she was operated under local anesthesia, with an intervening period of 3-6 months. In case of bony involvement, muscle island flaps such as pectoralis major and Latissimus dorsi were found to be excellent for interposition into new joints of the mandible to prevent re-ankylosis.[7] A high incidence of ankylosis was also noted in another study,[8] which had to be surgically corrected. There have been reports of using micro vascular free tissue transfer for restoration of defects caused by noma.[9] Our patient did not present with any major bony involvement and simple and short procedures were used effectively with suitable modifications and restored her facial defects quite aesthetically. REFERENCES
Copyright 2003 - Indian Journal of Plastic Surgery The following images related to this document are available:Photo images[pl03029f5.jpg] [pl03029f6.jpg] [pl03029s1-4.jpg] [pl03029f7.jpg] [pl03029f1-4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}