 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
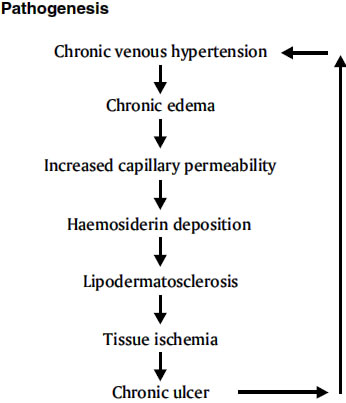
Indian Journal of Plastic Surgery, Vol. 37, No. 1, Jan-Jun, 2004, pp. 28-33 Original Article Role of free tissue transfer in management of chronic venous ulcer Reddy KMurali Mohan , Reddy DMukunda Department of Plastic Surgery, Nizams Institute of Medical Sciences Code Number: pl04006 ABSTRACT Most of the venous ulcers will heal with the treatment of primary venous problem. But a few patients will have refractory, recurrent chronic venous ulcers causing inconvenience to the patients in terms of loss of productive working hours. There is no standard method available for treatment of this chronic problem. Our modality of treatment includes wide excision of ulcer, ligation of incompetent perforators and coverage of defect with well vascularized tissue by free tissue transfer. We have analyzed this form of treatment in five patients with satisfactory result.INTRODUCTION Chronic venous ulcers affect 2% of adult population in Western countries. In India, statistics of this problem are not available. Magnitude of the problem may be higher due to various reasons. Chronicity of this problem may lead to prolonged periods of loss of man hour′s. Understanding of the pathogenesis of venous ulceration is incomplete. However, chronic venous hypertension[4] is thought to be a key cause that leads to the chronic venous insufficiency and ulceration. Because these lesions result from chronic venous hypertension, conventional management has focused at improving haemodynamics in the form of: 1. Local compression These techniques address haemodynamic disturbances but ignore other aspects of venous ulcerations, like surrounding lipodermatosclerosis[LDS] which is a scarred, poorly vascularised fragile tissue bed that is likely to ulcerate and is difficult to heal[5]. Most of the venous ulcers of short duration will heal with conventional treatments which focus on improving regional haemodynamics. These treatments however often fail to heal large recurrent venous ulcers that are associated with severe LDS. These refractory ulcers may occur in the following conditions:
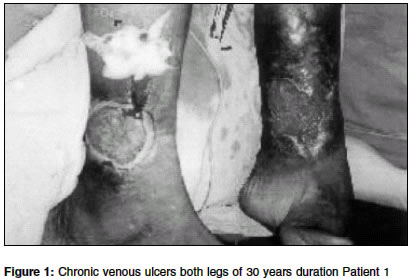
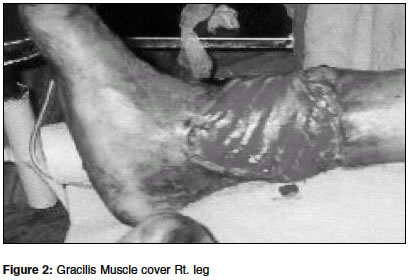
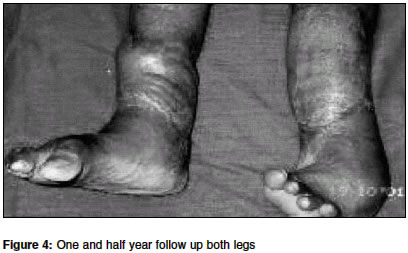
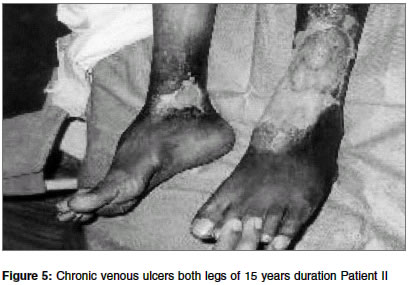
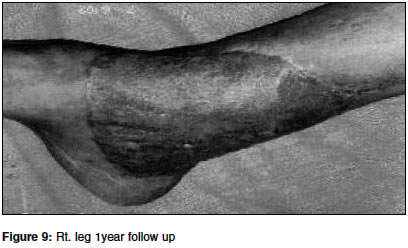
The end result of venous hypertension[5],[6] is a scarred, poorly vascularised large ulcer, often exposing vital structures like bones, tendons and joints. Commonly affected sites are lower half of leg and ankle on medial side. Often these ulcers are infected and are associated with secondary deformities of the ankle and foot. Optimum management of these ulcers includes: To prevent the recurrence of ulcer, wide excision of ulcer with surrounding LDS is required. The need for a large amount of well vascularised tissue and the location of these ulcers in the distal portion of the legs precludes the use of any local flaps. Many centers have reported the use of free tissue transfer in the form of muscle[6] and fasciocutaneous flaps[1] for these ulcers. Commonly used muscle flaps are Latissimus dorsi, Rectus Abdominis, Gracilis, Serratus anterior and fasciocutaneous flaps are Scapular flap and Anterolateral thigh flap. Major complications of free flap transfer in the treatment of venous ulcers are: 1. Increased risk of venous thrombosis especially in cases of Post DVT limbs. AIMS AND OBJECTIVES Aims and objectives of this study are to assess and evaluate the usefulness of free tissue transfer and morbidity associated with it for treatment of chronic large non healing venous ulcers. MATERIAL AND METHODS Five patients with large non healing venous ulcers of the leg were included in this study. The study was conducted from March 2001 to June 2002.The mean age of the patients was 46 years with a range 40-56 years. Out of the five patients four were males and one was female. Two patients had bilateral leg ulcers. Average duration of the ulcer was 12 years. Size of the ulcer ranged from100 to 300 cms2. All of them were located in the lower half of the leg and ankle. All the ulcers were recurrent with surrounding LDS changes. On an average each ulcer was treated thrice, by skin grafting. No patient had symptoms related to the DVT and arterial insufficiency. All the patients underwent some form of treatment for chronic venous insufficiency- three patients underwent saphenofemoral ligation and perforator ligation, one patient underwent only sub fascial ligation and sclerotherapy. In all the patients, the venous system was evaluated with color Doppler to asses the severity of venous reflux and to rule out deep vein obstruction. Two patients had sapheno femoral incompetence. All the patients had perforator incompetence. Two patients had deep vein reflux. PROCEDURE Excision of the entire ulcer along with surrounding LDS was done. Saphenofemoral ligation was done in two patients. Ligation of incompetent perforators was done in all the patients. Size of the defect after excision ranged from 150-500 cms2. In three patients tendons and bone were exposed after excision of the ulcer. Muscle flaps were chosen for free tissue transfer as all our patients had infected and large sized defects. Free omental transfer was done as a salvage procedure in a patient in whom free LD flap was lost. Total number of flaps 8 In six flaps, anastomosis was done to post tibial vessels and in the other two anastomosis was done to the anterior tibial vessels. All the anastomosis were end to end. Split thickness skin graft was applied over the flap immediately. COMPLICATIONS Major- two patients developed thrombosis of venous anastomosis in the immediate post operative period. One flap was salvaged by re-doing the anastomosis. In another patient who had deep vein reflux, the flap could not be salvaged. Subsequently after three days, free omental flap was done, which was also lost due to the venous problem. Finally wound was covered with skin graft. Minor- three patients developed minor graft loss and were managed conservatively with dressings. RESULTS Total number of patients 5 Follow-up Follow up ranged from 3 to 18 months. In the follow up of the patient who had lost two flaps and whose wound was managed with skin graft there was recurrence of ulceration after three months in the grafted site. One patient developed cellulitis in the leg around the flap after one month which was managed conservatively. No recurrence of ulcer was seen during 18 months follow-up period. All the patients were ambulant with elastic pressure garment support and returned to their original work. Patients with equinus deformity were referred to orthopaedic surgeons and physiotherapists for necessary treatment. DISCUSSION Chronic venous ulcer is a major health problem with considerable morbidity. Causes of these chronic recurrent ulcers include inadequate treatment of the primary venous problem and conservative approach on the part of treating surgeons in dealing with ulcers, like inadequate excision of ulcers and surrounding scarred unhealthy tissues. Adequate excision of these lesions will lead to defect which requires a large flap. As these ulcers are common in the lower leg and ankle local tissue transfer is often not possible, free tissue transfer is the only possible option. In these patients there are two specific complications while doing free tissue transfers, which are bleeding after excision leading to high chance of haematoma in the early post operative period and increased risk of thrombosis of venous anastomosis especially in post DVT limbs with and deep vein obstruction.[9] These patients require some form of venous reconstruction[5],[6] before planning for free tissue transfer. Therefore in our study all the patients underwent Doppler evaluation to rule out deep vein obstruction. In our study all the ulcers treated were chronic and refractory to the conventional treatment. Average duration of the ulcer was 12 years. Each patient underwent an average of three sittings of skin grafting per ulcer. All the ulcers were large and the defects after excision ranged from 100-500 cm2. The patients with chronic venous ulcers required an approach that addresses both venous hypertension and areas of ulcerative LDS. Conventional treatment strategies focus on improving regional venous haemodynamics but do not address severely diseased lipodermatosclerotic tissue. Our treatment strategy attempted to address both the problems. In our treatment protocol both the ulcer and the surrounding scarred, poorly vasculazised tissue were excised to prevent future ulceration. These defects are covered with healthy well vascularized tissue by means free tissue transfer. All the perforators were ligated during ulcer excision. In the later part of our series, to decrease the incidence of haematoma, free tissue transfer was done after 24 hours following excision of ulcer. In patients with severe venous reflux local heparinisation[3] was done with an in-situ venous cannula as a prophylactic measure to prevent thrombosis of venous anastomosis. Free muscle flaps contain numerous functioning micro-venous valves. These competent valves may contribute to improve local haemodynamics. In our series, six out of eight flaps were successful. Two flaps were lost in one patient in whom there was severe venous reflux as assessed by Doppler study. No recurrence of ulcer was noted in all the successful cases of free tissue transfer. In the long term follow up of similar studies from other centers,[6],[7] recurrence was noted in the same leg but not within the territory of transferred flaps. Reason for this ulceration is probably inadequate excision of surrounding LDS tissue. [Figure - 1], [Figure - 2], [Figure - 3], [Figure - 4], [Figure - 4], [Figure - 5], [Figure - 6], [Figure - 7], [Figure - 8], [Figure - 9] CONCLUSION Wide excision of the ulcer and surrounding LDS tissue combined with free muscle transfer is a useful adjunct to the conventional treatment of chronic venous ulceration and its recurrence. Although further work is required to determine the optimal indication for free flap procedures in chronic venous ulcers, we are encouraged by our results in providing our patients relief from chronic ulceration. ACKNOWLEDGEMENTS We are extremely thankful to Dr.R.Srikanth, Associate Professor, Dr. N. Ram Babu, Dr. V. G. Kishore, Assistant Professors and Dr.Subba Reddy, Post Graduate for their valuable suggestions on the subject. We are grateful to Mrs. V. Sujata for her help in the preparation of this paper. Last but not least we take this opportunity to thank all our patients without whom this study would not have been possible. REFERENCES
Copyright 2004 - Indian Journal of Plastic Surgery The following images related to this document are available:Photo images[pl04006f4.jpg] [pl04006f6.jpg] [pl04006f5.jpg] [pl04006f2.jpg] [pl04006f9.jpg] [pl04006f8.jpg] [pl04006f7.jpg] [pl04006f3.jpg] [pl04006f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}