 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
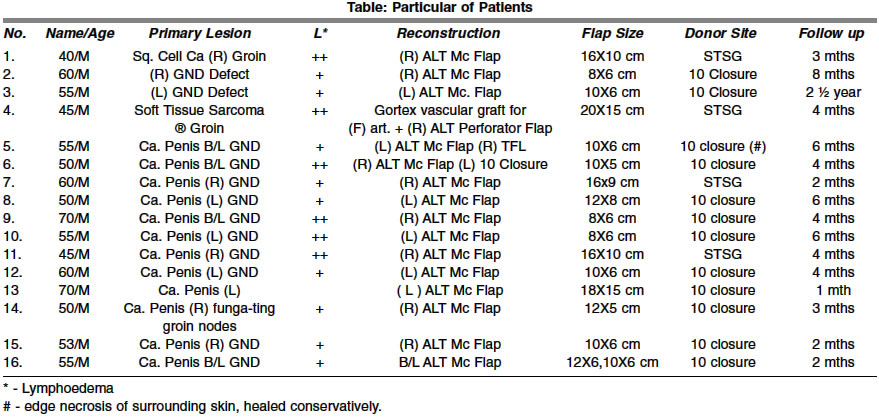
Indian Journal of Plastic Surgery, Vol. 37, No. 1, Jan-Jun, 2004, pp. 34-39 Original Article Groin reconstruction by anterolateral thigh flap: A review of 16 cases Quazi Ghazwan Ahmad ,Murali Reddy ,Kanti P Shetty , Rajendra Prasad , JS Hosi , M Bhathena Plastic & Reconstructive Services, Dept. of Surgical Oncology, Tata Memorial Hospital, Parel, Mumbai Code Number: pl04007 ABSTRACT We present our experience of pedicled Anterolateral thigh flap for reconstruction of groin defects in cancer patients. Total of 17 flaps in 16 patients were performed between January 2001 to May 2003. 15 flaps were used for groin defects after node dissection for carcinoma of Penis (bilateral groin defects in one patient), 1 case of Squamous Cell Carcinoma of groin and 1 case of Soft Tissue Sarcoma of groin. All patients were male. 16 were myocutaneous variety and 1 was fasciocutaneous flap based on the septocutaneous perforator. Complications were few and all patients achieved durable long-term coverage. We found the flap to be technically easy and reliable. Keywords: Groin Defects, Anterolateral Thigh Flap, Vastus Lateralis Muscle INTRODUCTION Exenterative pelvic surgery and groin dissection is commonly performed for cancer patients. Breakdown of wounds after inguinal block dissection is a common problem. Such wound margins are unhealthy and attempts at primary closure very often leads to failures. Fungating inguinal lymph nodes often require excision of skin and the resulting defect cannot be closed primarily. Coverage of such groin defects is an important and often difficult part of onco-reconstruction. Adequate and durable coverage of these defects is extremely important to prevent the exposure of femoral vessels which may lead to life-threatening blow-outs. Commonly used flaps for groin defect coverage are Tensor fascia lata, Gracilis, Rectus Abdominis, Rectus Femoris & Sartorius muscle flaps.[1],[2] Since Song et al.[3] reported the use of Anterolateral thigh flap (ALT flap) in 1984, this flap has been widely used in reconstructive procedures. After the initial reports of anatomic description and clinical applications of ALT flap from Asian countries, this flap gained popularity. This can be raised as an ultra thin perforator flap, thin fasciocutaneous flap, thick myocutaneous flap or may be combined with other flaps of the region to suit the requirements. Herewith we are presenting our experience of pedicled ALT flap for reconstruction of groin defects. We found it to be a reliable flap of good pedicle length; adjustable size, shape and volume and it can be combined with other local flaps (e.g. Tensor Fascia Lata flap, Rectus Femoris muscle flap). When the size of the flap was less than 8 cm in the transverse axis, primary closure of the donor site was possible. MATERIAL AND METHODS The duration of the study was from January 2001 to May 2003. 16 patients were included in this study and a total of 17 flaps were performed (bilateral in one case). [Table - 1]. Age group ranged from 35-70 years (Mean 53.2 yr.). All patients were male. Out of the 16 patients, 14 patients had defects secondary to groin node dissection for carcinoma Penis, one of them bilaterally. One patient underwent excision for fungating Squamous cell carcinoma of right groin and one other patient for soft tissue sarcoma of right groin. The size of the defect ranged from 8 x 6 cm. to 18 x 22 cm.16 defects in 15 patients were covered with Anterolateral myocutaneous flaps and in one case perforator based fasciocutaneous Anterolateral thigh flap was used. In all 16 Myocutaneous ALT flaps, only a portion of Vastus lateralis muscle, that was necessary to safeguard the musclocutaneous perforators, was included in the flap. The size of muscle included in the flap was always smaller than the size of skin paddle. In 13 cases, the donor site was closed primarily and in four cases of large defects, split thickness skin graft was required in addition. Relevant Anatomy
Operative Technique A portion of vastus lateralis muscle was included in all the flaps except in one case where the flap was based on one septocutaneous perforator. In one case of bilateral groin defects, on the opposite side tensor fascia lata flap was transposed [Figure - 3]. Primary closure of donor site was achieved in 13 cases and in four cases split thickness skin graft was used. Suction drain was used in all cases under the flap. Postoperative limb elevation was used and sutures were removed after about two weeks. RESULTS Satisfactory coverage of groin defects was achieved in all 16 cases. Out of the 13 cases of primary closure of donor site, 1 patient developed marginal necrosis of thigh skin flaps but settled without operative intervention. Overall 2 patients developed venous congestion of the flap and were explored on the first and second postoperative day respectively. In both the cases the pedicle was found to be compressed by one of the vascular pedicles of Rectus Femoris, which was divided, and the flap was salvaged completely. Rectus femoris muscle did not show any sign of vascular compromise on the table and both these patients did not have any problem of wound healing or any functional compromise subsequently. In net follow up of two months to 2½ years, all the flaps were well settled. Lymphoedema of the operated leg was noticed in all patients in the postoperative period, which was mild in ten cases and moderate in six cases. All patients were advised use of compression garments. None of our patients had any functional difficulty in walking or climbing stairs. The period of follow up mentioned in the table is the last time after operation that we saw the patient. The patients who have not been seen by us for longer period of time are either lost to follow up or have succumbed to their disease process. In view of the aggressive nature of their malignancies, we believe more in the latter of the two possibilities. DISCUSSION Reconstructive options for groin defects can be Sartorius, Gracilis, Rectus abdominis, Rectus Femoris, Tensor Fascia Lata muscle and myocutaneous flaps, Anterolateral thigh flap and local skin flaps.[2] Sartorius has a segmental blood supply (Type 4) and thin muscle belly, which is not suitable in many of the cases for the type of defect we need to cover. Skin availability is limited in Gracilis flaps and rectus abdominis myocutaneous flap leads to abdominal wall weakness. Tensor Fascia Lata flap creates unacceptable dog ears and there is need for skin grafting at donor site, while rectus femoris flap may cause weakness of knee extension. [Figure:2a] The requirements of the recipient site dictate the choice of flaps in a particular case. However, we have used the ALT flaps due to its advantages:
However, there are few disadvantages with the ALT flap:
Song et al in 1984 described the use of ALT flap as a free flap because of its inherent advantages.[3] In our cases due to the proximity of donor and recipient site, we are able to use the preferred free flap tissue as a pedicled flap. This ensures all the benefits of the free tissue transfer without the use of microsurgical tissue transfer techniques and its associated logistic problems. [Figure:2b] Kimata Y. et al[7] reported their experience of 74 cases where the ALT flaps were used successfully as pedicled flaps primarily for reconstructing groin and abdominal wall defects. In most of the cases they have used it as a fasciocutaneous flap while we have used it mainly as a musculocutaneous flap to meet the recipient site requirement. Sheng Kang Luo et al.[1] have demonstrated that ALT fasciocutaneous flaps can be used for difficult perineal and genital area reconstruction, especially scrotal reconstruction. This once again proves the versatility of pedicled ALT flaps as a reconstructive tool. Nobuyuki Yamada et al.[8] have suggested a new technique of flap elevation. They started simultaneous dissection with primary ablative surgery. They first marked the long medial incision, identified all skin perforators, then assessed the defect size and marked the primary flap and transposed it to cover the defect. The remaining skin with its identified perforators was used to close the donor defect in a V-Y manner without the help of skin graft. They found that this ensured better donor site management and faster and consistent surgery. However, we did not adopt this method as we feel that this increases the overall dissection and operative morbidity. Naohiro Kimura and Kaneshige Satoh[9] have demonstrated the technique of further thinning the ALT flap to a thickness that best suits the recipient site requirements. In our cases, however, we required a rather bulky flap so we have raised ALT as Myocutaneous flap in most of the cases. Perirong Yu et al.[10] have found that of the majority perforators, 2/3rd are musculocutaneous and only 1/3rd are septocutaneous. We had similar experience in our dissections and this is one of the reasons for doing ALT myocutaneous flaps in most of the cases. This increases the ease and reliability of the flap and makes the procedure much simpler. In two of our patients we had to divide one of the vascular pedicles to rectus femoris to relieve the compression on ALT pedicle. This was not associated with necrosis of rectus femoris muscle due to its accessory pedicles of vascular supply. Contrary to the earlier belief, the rectus femoris is a type II muscle with dominant pedicle branches from descending branch of lateral circumflex femoral artery. In addition to this there are multiple vascular pedicles from common trunk of ascending and transverse branches of lateral circumflex femoral artery and inferiorly from branches of femoral artery directly or via its branches to vastus medialis.[11],[12] In our experience of more than thirty cases of free ALT flap, we have witnessed more than one pedicle entering the rectus femoris muscle from the descending branch of lateral circumflex femoral artery. [Figure - 4] CONCLUSION To conclude, we feel that the anterolateral thigh flap is an attractive and reliable tool for reconstruction of complex groin defects. Technically the ALT myocutaneous flap is easy to harvest and meets the recipient site requirements adequately. Donor site morbidity is usually very little and manageable. Postoperative oedema usually responds to compressive garments. Long-term follow up reflects the robustness of the flap. REFERENCES
Copyright 2004 - Indian Journal of Plastic Surgery The following images related to this document are available:Photo images[pl04007t1.jpg] [pl04007f2a.jpg] [pl04007f1a.jpg] [pl04007f3.jpg] [pl04007f1b.jpg] [pl04007f2b.jpg] [pl04007f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}