 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
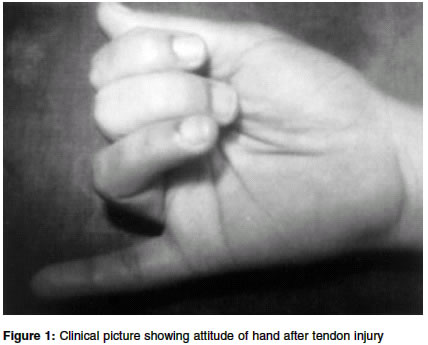
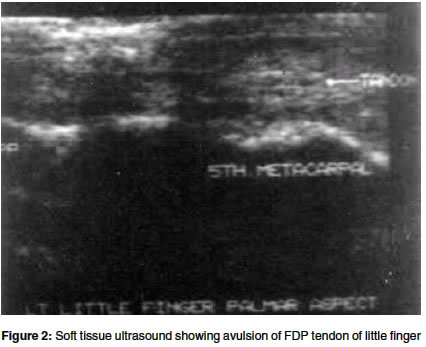
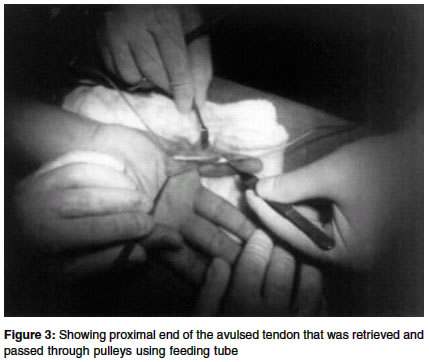
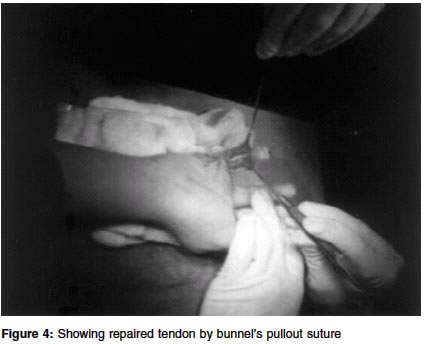
Indian Journal of Plastic Surgery, Vol. 37, No. 1, Jan-Jun, 2004, pp. 71-73 Case Report Closed rupture of the flexor digitorum profundus tendon of little finger: A case report Agarwal Pawan Plastic surgery unit, Department of Surgery, N.S.C.B. Government Medical College, Jabalpur - 482 003 Code Number: pl04015 ABSTRACT Closed rupture of the FDP tendon is rare. However, whenever they occur the most common site of rupture is the tendon-bone insertion, less frequent site is at the musculo-tendinous junction. Midsubstance ruptures are even more unique and are usually due to underlying pathology such as fracture, cystic degeneration, rheumatoid arthritis, or sequel following local steroid injection. This report describes a closed rupture of FDP tendon of little finger. Mechanism of injury, diagnosis and management are discussed. Keywords: Closed rupture, tendon INTRODUCTION Flexor tendon rupture in the palm is very infrequent. Unlike open tendon injuries, these injuries are often missed on initial presentation.[1] Early recognition and treatment can decrease the pain, dysfunction and long-term sequelae associated with these injuries. However, when they occur, the site of rupture is almost exclusively at the tendon-bone insertion and less frequently at the musculo-tendinous unit. Mid-substance ruptures are extremely rare and are usually due to an underlying cause such as fracture, cystic degeneration, rheumatoid arthritis, or sequelae following local steroid injection.[2] Less commonly, it may occur following nonunion of the hook of hamate, calcification of the triangular-fibro cartilage and non-specific synovitis.[3],[4],[5] The most common mechanism of injury for spontaneous rupture of the flexor tendons occurs when the hand is engaged in resisted flexion. Closed rupture of the tendon is unusual and such a case is being presented here. CASE REPORT A 23-year- old woman presented to the plastic surgery unit after injuring her right hand, which was engaged in resisted flexion. Physical examination of the right hand revealed tenderness over the proximal phalanx of the right fifth digit. The patient was unable to flex both distal and proximal interphalangeal joints of right little finger but had full range of motion of the metacarpo-phalangeal joint. [Figure - 1]. Neuro-vascular examination revealed intact function. As patient was unable to flex both distal and proximal interphalangeal joints of right little finger, clinical suspicion was avulsion of both the flexor tendons of little finger. Radiographic examination showed no fracture or dislocation. Soft tissue ultrasound using 10-megahertz probe demonstrated avulsion of FDP tendon from its insertion [Figure - 2]. The patient was taken to the operating room for exploration and repair of tendon under brachial block and tourniquet. A Bruner zigzag incision was made from proximal palmer crease to distal phalanx. Proximal end of the avulsed tendon was found at the level of the distal palmer crease and distally avulsed from its insertion. The flexor digitorum superficialis (FDS) tendon was intact. No evidence of tenosynovitis, cystic degeneration, or other abnormality was identified. Proximal end of the avulsed tendon was retrieved and passed through pulleys using feeding tube [Figure - 3]. Tendon repair was performed by bunnel′s pullout suture using 2-0 Prolene [Figure - 4]. A dorsal splint was used to immobilize the wrist for 3 week, with wrist flexion at 45 degrees and metacarpophalangeal joints (MPJs) at 90 degrees. A dynamic splint was then applied for active extension/passive flexion for an additional 3 weeks. Pullout suture was removed after 6 weeks. At 3 months, follow-up active range of motion for the MPJ was 0 to 70 degrees; proximal interphalangeal (PIP) joint, 0 to 60 degrees; and DIP, 0 to 40 degrees. Passive range of motion for the MPJ was 0 to 80 degrees; PIP, 0 to 90 degrees; and DIP, 0 to 60 degrees. DISCUSSION A closed rupture of a tendon may be defined as a rupture that occurs during movement and activity. Closed rupture of a flexor tendon is rare and ring finger is most commonly affected. Clinical observation of patients with this injury reveals that the ring fingertip is usually more prominent or "longer" than any other fingertip during grip in 90% of subjects and that it absorbs more force than any other finger during pull-away testing. Secondly the flexor digitorum profundus tendon, as demonstrated in cadaver specimens indicates a significantly weaker insertion of the ring finger compared to the middle finger.[6],[7] These factors contribute to the susceptibility of the ring finger to the profundus avulsion injury. In this case, on preoperative assessment in spite of intact flexor digitorum superficialis patient was unable to flex the proximal interphalangeal joint (PIP) joint, it was probably due to the reason that little finger superficialis is functionally deficient in approximate 33.8% of the normal population who could not achieve normal range of flexion at the proximal interphalangeal joint (PIP) This population is risk of complete loss of flexion at both interphalangeal joints in the event of isolated profundus disruption in the little finger.[8] The profundus tendon insertion on the distal phalanx is the usual site of injury and, as such, is appropriately termed as avulsion. In profundus avulsion injury, the traumatic agent is sudden extension while the finger is holding an object and the flexor digitorum profundus is strongly contracting. After avulsion tendon retracts and the stump can be found either at the distal pulley, or at the bifurcation of the superficialis tendon or in the palm of the hand.Leddy and Packer have described three types of profundus avulsions. In type I, the tendon retracts to the palm with disruption of the entire vincular system. Type II avulsion is characterized by retraction of the tendon to the PIP level that spares the vinculum longum. In type III, the profundus tendon avulsion occurs in addition to a fracture of the distal phalanx base. Rarely, a type III-A injury occurs, in which the tendon avulsion and fracture occur separately.[9] In cases of midsubstance rupture of an apparently normal flexor tendon the mechanism of injury is always forced flexion against resistance.[10],[11] Localizing the level of the tendon rupture can be a difficult task. MRI allows for accurate preoperative assessment of tendon position and degree of retraction, thereby facilitating surgical planning and approach.[12] MRI is a costly investigation and may not available everywhere in developing country. Therefore we have used soft tissue ultrasound (10 megahertz probe) for localization of avulsed tendon. Accurate localization of tendon pathology preoperatively minimizes unnecessary dissection, shortens the operative procedure, and clarifies operative planning.[13],[14] Avulsion of flexor digitorum profundus (FDP) is classically repaired to the base of the distal phalanx via a pullout suture over a button with good results but in cases of delayed diagnosis, such as happens in 75% of cases the treatment can be difficult and sometimes arthrodesis of the distal interphalangeal joint is the only possible therapy. REFERENCES
Copyright 2004 - Indian Journal of Plastic Surgery The following images related to this document are available:Photo images[pl04015f3.jpg] [pl04015f2.jpg] [pl04015f4.jpg] [pl04015f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}