
|
Indian Journal of Plastic Surgery
Medknow Publications on behalf of Indian Journal of Plastic Surgery
ISSN: 0970-0358 EISSN: 1998-376x
Vol. 37, Num. 2, 2004, pp. 99-104
|
Indian Journal of Plastic Surgery, Vol. 37, No. 2, July-December, 2004, pp. 99-104
Original Article
Correlation of renal complications with extent and progression of tissue damage in electrical burns
D. C. Chauhan, P. S. Chari, G. K. Khuller*, Dalbir Singh**
Departments of Plastic Surgery, *Biochemistry and **Forensic Medicine, Post Graduate Institute of Medical Education and
Research, Chandigarh, India.
Address for correspondence: Dr. D. C. Chauhan, c/o Dr. S. Makkar, Asstt. Professor, Department of Plastic Surgery, PGIMER,
Chandigarh, India. E-mail: dcchauhan@sancharnet.in
Code Number: pl04023
Abstract Electrical injuries due to high-tension voltage (>1000 volts) cause destruction at the point of contact with massive necrosis of deeper structures such as muscles, vessels and nerves. Rhabdomyolysis due to massive breakdown of skeletal muscles may lead to acute renal failure secondary to myoglobinuria. The study was undertaken to observe the correlation of renal complications with extent and progression of tissue damage in high-tension voltage electrical burns. Renal biochemical parameters as predictors of acute renal failure were also studied. Thirty two patients of high tension voltage electrical burn injuries presenting during one year period 1-1-2001 to 31-12-2001 were studied. Low-tension voltage electrical injuries (<1000 volts) mimic thermal burns were excluded from the study. The electrical wound assessment and the renal biochemical parameters were done daily for the first seven days and then on alternate days for another seven days. Assessment of progression of wounds and correlation with the renal biochemical parameters was done. Patients who died following electrical burns were subjected to autopsy and histopathological examination of both kidneys. Out of the thirty-two patients, six (18.75%) went into acute renal failure. Five out of these six patients died because of renal failure (mortality rate 83.33%). There was definite progression of electric burn wounds. There was no correlation between progression of electrical burn wounds and acute renal failure. Serum creatinine was found to be the most important biochemical parameter as a prognostic indicator of acute renal failure.
Keywords: Electrical Burns, Renal Failure, Renal Biochemical Parameters
INTRODUCTION
Electrical burns accounts for 3% - 4% of all admissions to burn units.[1] In high-tension voltage electrical injury, there is deep ′hidden′ destruction of muscular structures beneath apparently uninvolved skin. Rhabdomyolysis due to massive break down of skeletal muscles in electrical injuries may lead to acute renal failure secondary to myoglobinuria.[2] In the literature there is controversy regarding progression of electrical burn wound, correlation of renal complications with tissue damage in electrical burns and the mechanism by which renal failure occurs following rhabdomyolysis induced by electrical injury.[3]
The purpose of this study was to correlate the renal complications with extent, depth and progression of tissue damage in high tension voltage electrical burns.
MATERIALS AND METHODS
Thirty-two patients with high tension voltage (>1000 volts) electrical burns who reported to the Plastic Surgery Department, PGIMER, Chandigarh during the year 2001 formed the study group. Patients presenting later than a week of electrical burns, or those with low-tension voltage electrical burns were excluded from the study. Patients with known history of chronic renal disease or existing co-morbid conditions such as diabetes mellitus, hypertension, were not taken into the study. All the patients were evaluated by detailed history and clinical examination. Proper fluid resuscitation and other preventive measures against acute renal failure were taken as follows. Resuscitation involved infusion of crystalloid at 4 ml/kg/% total body surface area burn (TBSA) which was increased to 9 ml/kg/% total body surface area to maintain urine output of 1-2 ml/kg/hr.[5] Mannitol 12.5 gm/hr was used to maintain the urine output of 1-2 ml/kg/hr whenever indicated. In cases of metabolic acidosis alkalinsation of blood was done by infusing 50 ml of 7.5% sodium bicarbonate (45 meq) and repeated whenever required.
Acute renal failure was defined as elevation of serum creatinine to above 2 mg/dl (177 µmol/L) in patients with normal baseline serum creatinine (< 1.5 mg/ dl).[6] Urine output was recorded every hour for the first three days since the time of burns and then daily for another eleven days. Renal function tests included serum creatinine, potassium, bicarbonate, blood urea and pH daily for seven days since burns and then alternate day for another seven days. Creatine phosphokinase MM, serum myoglobin and urine myoglobin were done on first and second day burns. Cultures from blood, urine and wound were sent weekly for first two weeks. Peak high values were noted of all the parameters.
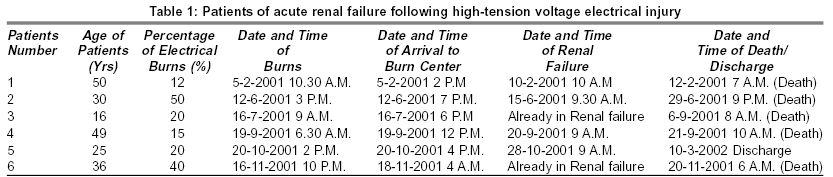
[Table - 1] depicts the details of all the six patients out of thirty-seven who went into acute renal failure. In four out of six patients that went into acute renal failure, the referral record from the referring hospital showed that proper fluid resuscitation and other preventive measures against acute renal failure were taken from time of electrical injury to arrival to our burn center. In two patients, the referral records revealed that adequate measures were not taken and on their arrival to burn center, they were already in acute renal failure.
Electric burn wounds were debrided daily and cleaned with normal saline followed by silver sulphadiazine ointment application to the wounds. It was covered with gauze, cotton pads and then bandaged. Length and breadth of all wounds on the surface was measured (cm2) to know its extent. The depth of wounds was also measured which was categorized as 2o-partial thickness, 3o-full thickness, 4o-muscle or bone deep burns. These wounds were measured daily for seven days and then on alternate days for another seven days. After serial debridements and dressings leading to healthy wound, it was covered with split skin graft or flap cover and at times when the wound was not salvageable in limbs, amputation of the part was done.
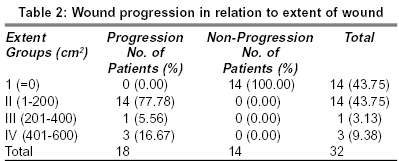
Progression of wounds, in both cases of extent and depth, is the difference in the surface area involved in a patient at the time of first examination on arrival in hospital and last value on fourteenth day or at the time of amputation of the gangrenous burnt part or death of the patient. These wounds showed progression or increase both in terms of extent (burned body surface area) and depth. [Table - 2] shows wound progression in relation to extent of wound, column one shows the categorization of wounds into four groups depending upon the extent of wound. Column two shows that eighteen out of thirty-two patients had progression to variable extent as seen in numbers and corresponding percentage. Column three shows the numbers and percentage of the fourteen patients who did not show any progression.
Twenty eight patients sustained electrical burn injury on one or more limbs to variable extent and degrees, and fasciotomy was given to relieve the compartment syndrome and was also used to assess the status of underlying muscle and to note progression of muscle necrosis. On other parts of body, fasciotomy was not done and wound assessment was done with the help of debridements as fasciotomy though helpful also increases morbidity.
In case of death following electrical burns medico legal autopsy was conducted. Gross findings of the kidneys were noted. Specimens from both kidneys were microscopically examined and the findings recorded.
RESULTS
Thirty-two patients with high-tension voltage electrical burns presented during one year of study. Mean age at presentation was 29 years with the range of 9-54 years. Thirty patients were males and two were females. Mean total body surface area of electrical burns was 20.59% with range being 3-50%. Mean hospital stay was 40.38 days with a range of 2-140 days.
Electrical burns sustained by patients were either contact burns or flash burns or both. Contact burns with third degree and fourth degree deep burns showed progression of electrical wounds. Out of thirty-two patients, eighteen patients showed progression of wounds in relation to extent of the wounds [Table - 2]. Third degree deep wounds were present in nineteen patients and all the wounds progressed. Fourth degree deep burns were present in fifteen patients and all of them progressed [Table - 3].
Out of six patients who went into renal failure, five showed progression of wounds both in extent and depth. [Table - 4] and [Table - 5] In one patient progression of wounds could not be assessed as the patient presented late by about thirty hours with acute renal failure and died in fifty hours on arrival to burn center.
Nine patients not developing renal failure, showed progression of wound in relation to extent of wounds [Table - 4] Progression of wound in relation to third degree burns was observed in fourteen patients and fourth degree burns was seen in ten patients [Table - 5].
In all thirty-two patients, eight renal parameters were studied. They were blood urea, serum creatinine, potassium, bicarbonate, pH, creatine phosphokinase MM, myoglobin and urine myoglobin [Table - 6]. These parameters were deranged in all six patients, who went into renal failure. In twenty-six patients who did not develop renal failure, one to seven out of eight renal biochemical parameters were deranged. Serum creatinine was not raised in any of the patients. Serum potassium was raised in two patients and blood urea was raised in fourteen patients. Bicarbonate levels were below normal in twenty-five patients, and pH was acidic in thirteen patients. Creatine phosphokinase MM was raised in twenty-three patients, serum myoglobin was raised in twenty-three patients and urine myoglobin was positive in five patients.
[Table - 1] depicts the details of all the six patients out of thirty-two who went into acute renal failure. Electrical injuries in these patients were caused by high-tension voltage. Age of patients ranged from sixteen to fifty years. Patients reported to our burn center within few hours of electrical injury, one patient reported about thirty hours late. Two patients out of the six were in acute renal failure at time of reporting, the remaining patients developed renal failure at variable periods ranging from one to eight days. Daily serum creatinine levels of these six patients going into renal failure from 1-13 days has been shown in [Table - 7]. Five out of these six patients died due to acute renal failure inspite of all resuscitative measures including multiple peritoneal dialyses. Four of them underwent medico legal autopsy and the kidney tissue was subjected to histhopathological examination, which showed evidence of acute tubular necrosis of varying degrees. Predominant finding was tubular degeneration tubulorrhexis and focal areas of tubular regeneration in some cases. Heme casts were prominent in all four cases of renal failure. Interstitium showed focal lymphocytes infiltration in all four cases of acute renal failure.
DISCUSSION
There was progression of electrical wounds in extent and depth. In 83.3% of patients who went into acute renal failure in our study showed progression in extent and third degree and fourth degree deep burns wounds. The patients who did not go into acute renal failure, progression was observed in extent in 42.3% and progression was seen in third degree and fourth degree deep burn wounds in 53.8% and 38.4% patients respectively. Therefore no correlation between acute renal failure and wound progression could be drawn.
Controversy exists regarding progression of electrical burn wounds. Proponents of the theory of progression suggest that progressive necrosis in electrical wounds is due to thrombosis resulting in injured vessel due to heat,[7] release of arachadonic acid metabolites from the periosseous musculature,[8] bacterial infection,[9] or decreased vascularity from small vessels thrombosis.[10]
Those contradicting this theory of progression of electrical wounds are Hunt et al[11] who reported immediate vascular occlusion in the hind limbs vessels corresponding to cutaneous and muscular injury. No evidence of progressive vascular occlusion was identified in his angiographic study. Zelt et al[12] in their experimental study of electrical burns wound observed that there was no progression and the demarcation between viable and non viable muscles and remained unchanged up to ten days after injury.
The reported incidence of acute renal failure following electrical burn wounds is 1.5-7.5%[13] Arturson et al[14] reported acute renal failure in seven out of fifty patients of high tension electrical injury and four of them died. In a study by Baxter et al[7] two patients went into acute renal failure out of forty patients of electrical burns. Bajaj et al[15] reported acute renal failure in thirteen out of one hundred and ten patients and five died.
In our study the incidence of acute renal failure was 18.75%, one of the possible causes for such high incidence was delayed presentation and inadequate resuscitation during transit in two patients who were already in acute renal failure on arrival to burn center and severity of electrical injury. Age of these patients ranged from 16-50 years which was unlikely to predispose to acute renal failure. None of the patients was on nephrotoxic drugs prior to electrical injury. Cardiovascular status of these patients on presentation was altered in form of tachycardia, hypotension and tacaponea for which appropriate steps were taken. Wound management included serial debridements once daily, at times amputations of non- salvageable parts to reduce necrotic muscle mass. Three of the above patients going into acute renal failure underwent amputations of one of the limbs.
All the six patients going into acute renal failure showed altered values of the eight biochemical parameters studied. Patients who did not go into renal failure had one to seven altered renal parameters out of eight renal parameters [Tabe - 6]. Serum creatinine was found to be the most important prognostic indicator for patients going into acute renal failure followed by serum potassium. Our study also showed similar findings of serum creatinine as shown in [Table - 7]. In acute renal failure following high-tension voltage electrical burns raised creatinine and potassium levels has been reported and is an indication for dialysis.[6],[16] Blood urea is not an useful independent indicator as it is increased in non renal conditions such as dehydration and high protein diet. Low serum bicarbonate levels and low blood pH are also not prognostic though it has been suggested that low venous bicarbonate levels < 17 mmol/L in patients with myoglobinurea were predictors of acute renal failure.[1],[17]
In patients with rhabdomyolysis progressing to renal failure blood pH tended to be significantly more acidemic.[18] Creatine phosphokinase MM levels did not contribute additional predictive value in our patients with renal failure, though it had been reported by Schulze et al[19] that increasing and decreasing levels provided some insight into whether rhamdomyolysis was increasing or resolving. Myoglobinurea as compared to serum myoglobin has been reported to be an indicator of patients going into acute renal failure.[20] In our study 45% of the patients having myoglobinurea developed acute renal failure, corroborating to other studies that not all episodes of rhabdomyolysis with myoglobinurea lead to renal failure.[3],[21] Obstructive cast formation because of filtered myoglobin precipitation as an etiological factor in acute renal failure is facilitated by hypovolemia, blood acidemia and acidic concentrated urine.[22],[23] A patient with superficial electrical burns does not develop myoglobinurea but in full thickness burns there is a risk of myoglobinurea in 27% patients.[1] Incidence of myoglobinurea after electrical injury in our study was 34.3% whereas in literature it has been reported to be 14-42%[24] and had been said to be as high as 75-100%.[25]
Mortality in patients going into acute renal failure in our study was five out of six (83.3%). Histopathological features of the kidney tissue obtained on postmortem showed definite changes of acute renal failure secondary to myoglobinuria following rhabdomyolysis due to high tension voltage electrical injury. Ante- mortem renal biopsy may help us in early diagnosis of acute renal failure but whether this invasive procedure will be a better prognostic indicator than clinical and biochemical parameters and whether it will be feasible and ethical in acute sick patients of electrical burns, needs to be further examined.
Our study showed that there was definite progression of electric burn wounds. There was no correlation between progression of electrical burns wounds and acute renal failure. Of the biochemical parameters, serum creatinine was found to be the most important prognostic indicator of acute renal failure.
References
| 1. | Rosen CL, Adler JN, Rabban JT, et al. Early predictors of myoglobinuria and acute renal failure following electrical injury. J Emerg Med 1999;17:783-9. Back to cited text no. 1 [PUBMED] [FULLTEXT] |
| 2. | Bingham H. Electrical burns. Clin Plast Surg 1986;13:75-84. Back to cited text no. 2 |
| 3. | Gabow PA, Koehny WD, Kelleher SP. The spectrum of rhabdomyolysis. Baltimore: Medicine 1982. p. 61:141. Back to cited text no. 3 |
| 4. | Robson MC, Smith DJ. Care of the thermally injured victim. In: Jurkiewicz MJ, Krizek TJ, Mathes SJ, Ariyan S, editors. Plastic Surgery: Principles and practice. St Louis: CV Mosby Company; 1990. p. 1355-410. Back to cited text no. 4 |
| 5. | Luce EA. The spectrum of electrical injuries. In: Lee RC, Cravalho EG, Burke JF, editors electrical trauma, New York: Cambridge University Press; 1993:106. Back to cited text no. 5 |
| 6. | Jha V, Malhotra HS, Sakhuja V, Chugh KS. Spectrum of hospital acquired acute renal failure in the developing countries. Chandigarh Study. QJ Med 1992;303:497-505. Back to cited text no. 6 |
| 7. | Baxter CR. Present concept in the management of major electrical injuries. Surg Clin North Am 1970;50:1401-18. Back to cited text no. 7 [PUBMED] |
| 8. | Robson MC, Murphy RC, Heggers JP. A new explanation for the progressive tissue loss in electrical injuries. Plast Reconstr Surg 1984;73:431-7. Back to cited text no. 8 [PUBMED] |
| 9. | Muir IFK. The treatment of electric burns. Br J Plast Surg 1958;10:292. Back to cited text no. 9 |
| 10. | Wilkinson C, Wood M. High voltage electric injury. Am J Surg 1978;36:693. Back to cited text no. 10 |
| 11. | Hunt JL, McManus WF, Hanlay WP, Pruitt BA. Vascular lesions in acute electrical injuries. J Trauma 1974;14:461-73. Back to cited text no. 11 |
| 12. | Zelt RG, Daniel RK, Ballard PA, Brisette Y, Heroux P. High voltage electrical injury: Chronic wound evolution. Plast Reconstr Surg 1988;82:1027-41. Back to cited text no. 12 |
| 13. | Solem L, Fischer RP, Strate RG, Natural history of electrical injury. J Trauma 1977;17:487-92. Back to cited text no. 13 |
| 14. | Arthurson G, Hedlund A, Primary treatment of 50 patients with high tension electrical injuries. Scand J Plast Reconstr Surg 1984;18:111-8. Back to cited text no. 14 |
| 15. | Bajaj SP, Tiwari VK, Kohli JS, Pande S. Profile of electrical burns admitted in burns unit of Safdarjang hospital. Indian J Burns 1998;6:31-4. Back to cited text no. 15 |
| 16. | Zager RA. Studies of mechanism and protective maneuvers in myoglobinuric acute renal injury. Lab invest 1989;60:619. Back to cited text no. 16 [PUBMED] |
| 17. | Muckart DJJ, Moodley M, Naidu AG, Reddy ADR, Meineke KR. Prediction of acute renal failure following soft tissue injury using the venous bicarbonate concentration. J Trauma 1992;33:813-7. Back to cited text no. 17 |
| 18. | Ward MM. Factor predictive of acute renal failure in rhabdomyolsis. Arch Intern Med 1988;148:1553. Back to cited text no. 18 [PUBMED] |
| 19. | Schulze VE Jr. Rhabdomyolysis as a cause of acute renal failure. Postgrad Med 1982;72-145. Back to cited text no. 19 |
| 20. | Clyne DH, Kant KS, Pexe AJ, Pollack VE, Nephrotoxicity of low molecular weight serum proteins. Physiochemical interactions between myoglobin, hemoglobin, Bence Jones proteins and Tamm Horsfall mucoprotein. Curr Prob Clin Biochem 1979;9:299. Back to cited text no. 20 |
| 21. | Gupta KL, Kumar R, Shekhar MS, Sakhuja V, Chugh KS. Myoglobulinuric acute renal failure following electrical injury. Ren Fail 1991;13:23-5. Back to cited text no. 21 |
| 22. | Bywaters EGL, Stead JK, The production of renal failure following injection of solutions containing myohaemoglobin. QJ Exp Physiol 1944;33:53. Back to cited text no. 22 |
| 23. | Feinfeld DA, Cheng JT, Beysolow TD, Briscoe AM. A prospective study of urine and serum myoglobin levels in patients with acute rhadbomylosis. Clin Nephrol 1992;38:193-5. Back to cited text no. 23 [PUBMED] |
| 24. | Hunt JL, Sato RM, Baxter CR, Acute electrical burns. Current diagnostic and therapeutic approaches to management. Arch Surg 1980;115:434-8. Back to cited text no. 24 |
| 25. | Luce EA, Gotilieb SE. True high tension electrical injuries. Ann Plast Surg 1984;12:321-6. Back to cited text no. 25 |
Copyright 2004 - Indian Journal of Plastic Surgery
The following images related to this document are available:
Photo images
[pl04023t6.jpg]
[pl04023t3.jpg]
[pl04023t1.jpg]
[pl04023t4.jpg]
[pl04023t7.jpg]
[pl04023t5.jpg]
[pl04023t2.jpg]
|

{kind=link}
{kind=link}
![[Table - 3]](/showimage?pl/photo/pl04023t3.jpg){kind=link}
![[Table - 4]](/showimage?pl/photo/pl04023t4.jpg){kind=link}
![[Table - 5]](/showimage?pl/photo/pl04023t5.jpg){kind=link}
![[Table - 6]](/showimage?pl/photo/pl04023t6.jpg){kind=link}
![[Table - 7]](/showimage?pl/photo/pl04023t7.jpg){kind=link}