 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
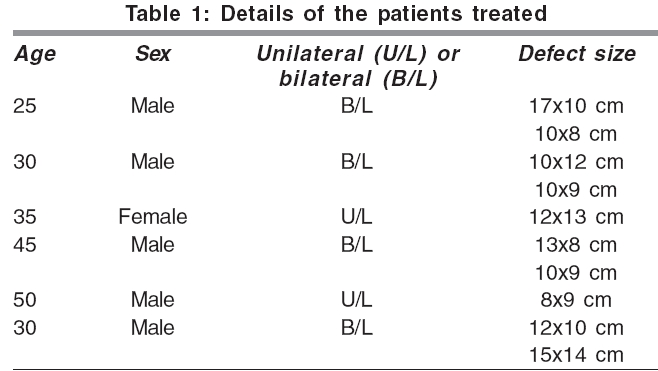
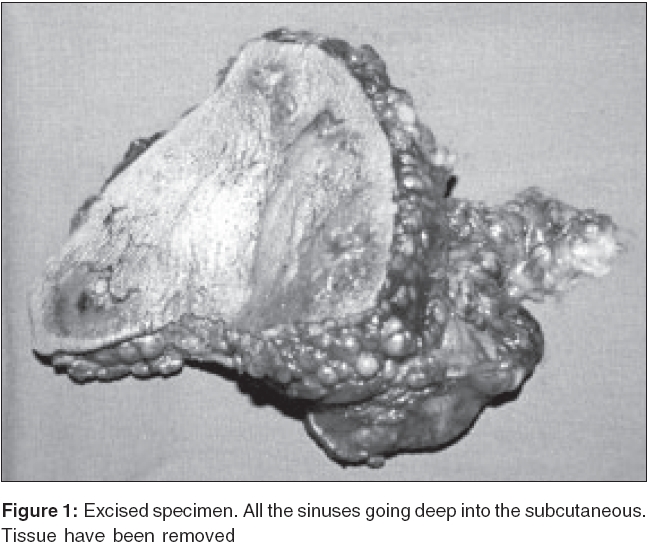
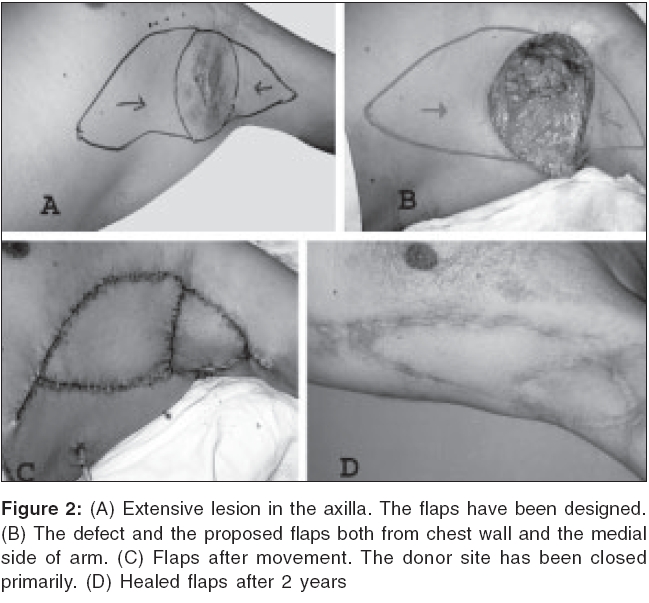
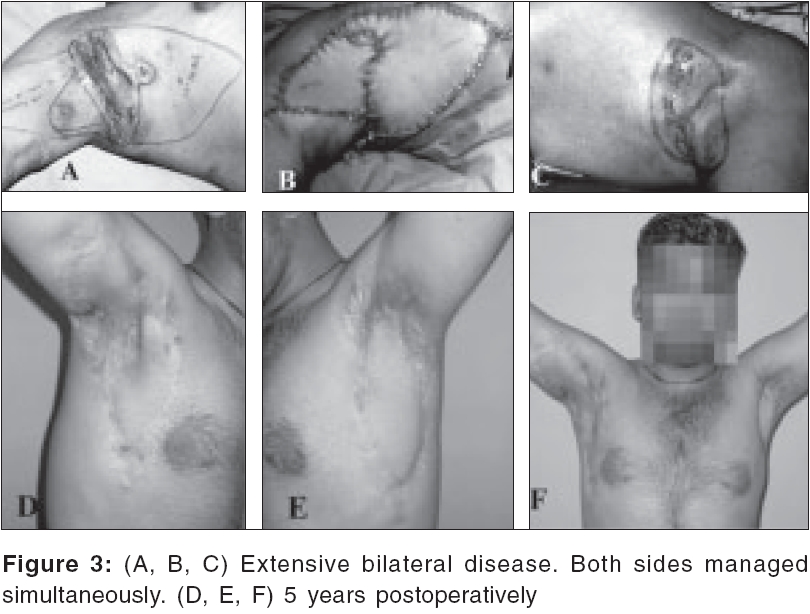
Indian Journal of Plastic Surgery, Vol. 39, No. 1, January-June, 2006, pp. 18-21 Original Article Reconstruction in extensive axillary Hidradenitis suppurativa with local fasciocutaneous V-Y advancement flaps Ramesh Kumar Sharma, Krishan Mohan Kapoor, Gurpreet Singh* Departments of Plastic Surgery and *General Surgery, Postgraduate Institute of Medical Education and Research, Chandigarh, India Code Number: pl06005 Abstract We present our experience with the use of local fasciocutaneous V-Y advancement flaps in the reconstruction of 10 axillae in 6 patients for large defects following wide excision of long-standing Hidradenitis suppurativa of the axilla. The defects were closed with local V-Y subcutaneous island flaps. A single flap from the chest wall was sufficient for moderate defects. However, for larger defects, an additional flap was taken from the medial side of the ipsilateral arm. The donor defects could be closed primarily in all the patients. The local areas of the lateral chest wall and the medial side of the arm have a plentiful supply of cutaneous perforators and the flaps can be designed in a V-Y fashion without resorting to preoperative marking of the perforator. The flaps were freed sufficiently to allow adequate movement for closure of the defects. Although no attempt was made to identify the perforators specifically, many perforators were seen entering the flap. Some perforators can be safely divided to increase reach of the flap. All the flaps survived completely. A follow up of 2.5 years is presented. Keywords: Hidradenitis suppurativa , axillary full thickness skin defects, fasciocutaneous v-y flap, lateral chest wall, medial arm INTRODUCTION Hidradenitis suppurativa of the axilla is a very frustrating condition and can follow an indolent course causing serious morbidity in the patients. Surgical excision is the best method of treatment in chronic cases of axillary Hidradenitis suppurativa . Although a number of surgical options have been used, wide surgical excision is considered the best option with a minimal likelihood of recurrence.[1] Cover of excision defects with skin grafts can result in unfavorable aesthetic and functional results with possible shoulder joint rehabilitation problems including contracture of the axilla.[2] Local fasciocutaneous flaps can provide thin, pliable skin that allows early return of shoulder joint function. We describe the use of a local fasciocutaneous V-Y advancement flap from the lateral chest alone or in combination with a medial arm fasciocutaneous V-Y advancement flap for coverage of axillary defects in cases of Hidradenitis suppurativa .MATERIALS AND METHODS In the last 5 years we have treated 10 axillae in six patients with chronic indolent Hidradenitis suppurativa of more than three years duration. All these patients were referred by dermatology colleagues after failure of conservative medical treatment. The male to female ratio was equal. All patients were treated by radical surgical excision. The size of the defects created after excision of the lesions ranged from 80 cm 2 to 210 cm 2 [Table - 1]. The sinus tracts were going deep into the fat up to the deep fascia. The entire involved skin, axillary fat and deep fascia was excised. In almost all the cases the axillary vessels were bared. The closure of defects was achieved by fasciocutaneous V-Y advancement flaps taken from the local tissue. In smaller defects a single flap from the lateral chest wall was enough. However, in extensive cases an additional flap was taken from the medial arm. Four of the patients had bilateral disease while two had unilateral disease. Radical excision was performed after at least 2 years of recurrent disease. In 7 out of total 10 axillae operated, a combination of lateral thoracic and medial arm fasciocutaneous V-Y advancement flaps was used. In bilateral cases, simultaneous surgery was performed on both the sides. Shoulder movements were started on the second postoperative day. The duration of follow up ranged from 2 to 5 years. Anatomy Several vessels richly supply the skin in the region of the medial surface of the arm and the lateral thoracic wall, making these areas ideal to raise thin subcutaneous flaps. The lateral chest wall is supplied by multiple direct cutaneous perforators from the subscapular-thoracodorsal arterial axis, lateral thoracic artery and the pectoral branch of the acromio-thoracic artery.[3],[4],[5],[6] The skin on the medial aspect of the upper arm is supplied by a series of five to six fasciocutaneous perforators which arise from the brachial artery, from its branches to biceps, from the superior ulnar collateral artery and when present, middle ulnar collateral artery. These perforators emerge along the medial intermuscular septum and fan out over the biceps and the triceps at the level of the deep fascia. These perforators supply the flaps in this region and the anastomosis between successive perforators facilitates blood flow along the long axis of the flap.[7] Surgical technique In all patients, Hidradenitis suppurativa was treated by surgical excision of the diseased tissue that included all of axillary hair bearing skin along with the involved apocrine glands. Skin along with 1-2 cms thick subcutaneous layer of adipose tissue, underlying lymph nodes and sometimes fascia were included in the specimen as the overlying skin was adherent to these due to fibrosis resulting from recurrent chronic infection [Figure - 1]. The dissection superficial to axillary vessels was difficult in all the cases, due to extensive fibrosis. In all cases, the excision resulted in the exposure of axillary vessels necessitating the coverage of defect with a flap. The resultant defects had a shape similar to a rhomboid, the widest part of the defect being at the axillary dome. A triangular flap was marked on the lateral thoracic wall with the base formed at the lower border of the axillary defect [Figure - 2]A, B and [Figure - 3]A, B. The base of the flap was equal to the maximum width of the axillary defect. Incisions on anterior and posterior borders of the flap were taken through the skin and deep fascia and the flap was mobilized. The flaps were mobilized, sufficiently maintaining as much attachment as possible. No attempt was made to look for any perforators. The flap was moved like a V-Y advancement flap into the defect in the axilla. The donor defect was closed by direct suturing [Figure - 2]C. The healing was uneventful and the flaps maintained the contour of the axilla well [Figure - 2]D. In cases where the defect extended on to the medial aspect of the arm and which could not be closed primarily, another V-Y advancement flap from the medial surface of the arm was raised and inserted into the remaining defect. The closure was done in two layers; subcutaneous tissue with 3-0 chromic catgut and skin with 3-0 nylon and skin staplers. A suction drain was kept in all cases and was generally removed 3-4 days later, when the drainage decreased to about 30 cc in 24 hours. The skin sutures were removed after 10 days in all patients. Even in extensive disease in bilateral cases, simultaneous management could be done with primary closure on both sides with satisfactory long term results [Figure - 3] A-F. RESULTS All flaps healed without complications. During follow up, there was no disease recurrence or scar contracture. The mean postoperative stay in the hospital was 5 days. Physiotherapy was started from the second postoperative day and no patient had any impairment of shoulder joint movement. The cosmetic results of the reconstructed area were satisfactory. The lack of hair bearing skin in axillae was not a complaint as the patients were happy to get rid of the disease. The aesthetic results of donor areas were also satisfactory as both the scars were in hidden areas.DISCUSSION Hidradenitis suppurativa is an annoying chronic condition characterized by swollen, painful, inflamed lesions in the axillae, groin and other parts of the body that contain apocrine glands. The disease is a chronic acneiform infection of the cutaneous apocrine glands that also can involve adjacent subcutaneous tissue and fascia. The condition occurs when gland outlets become blocked by perspiration or are unable to drain normally because of incomplete gland development. Secretions trapped in the glands force perspiration and bacteria into surrounding tissue, causing subcutaneous induration, inflammation and infection. The axilla is very commonly involved. Hidradenitis suppurativa initially presents with deep-seated nodules, which coalesce and get infected to form acute abscesses. It may progress to chronic sepsis with sinus and fistula formation, multiple abscesses and extensive dermal scarring.[8] The goals of surgical management are to (1) completely excise all the involved tissue, (2) preserve function, avoiding development of axillary contracture and (3) obtain satisfactory aesthetic results. The extent of skin excision has a major role in determining the recurrence rate. In one study,[7] 27% of the patients treated by local excision of only the involved skin had recurrent disease, whereas only 7% patients had recurrence with excision of hair bearing skin and none had recurrence with wide local excision of skin. Skin grafting to cover the resulting defect has its limitations. It is not a good choice because of poor vascularity and bacterial contamination of the subcutaneous fat leading to failure of complete graft take. Splintage of the axilla with shoulder in abduction is uncomfortable especially in bilateral axillary excision.[1] Further, after skin grafting the patient can develop shoulder joint stiffness because of immobilization.[2] In most cases, excision of the involved area leads to exposure of axillary vessels which preferably require a flap cover. Other problems associated with skin grafting are poor aesthetic appearance, hyper-pigmentation and dryness. The ideal method for resurfacing a defect near a joint is coverage with a flap.[9],[11],[12] The flap can be raised from local areas without any need to change the position of the patient as in parascapular flap. The blood supply is constant and can be further ascertained by picking up perforators with Doppler studies. The donor site can always be closed primarily. In case the defect is too extensive, another V-Y flap can be very easily raised from the medial aspect of arm based upon the copious perforators in this region. Although some authors have suggested dissection of the individual perforators for better reach of the flaps for axillary defects in hidradenitis ,[10],[13] we have achieved sufficient movement of the flaps without resorting to dissection of perforators. The flaps are very thin and so can very easily fit into the contours of the axilla. The vascularized flaps help in better control of infection and invariably healing is primary in all the patients. The patient can start using the shoulders immediately which is a great bonus in cases where bilateral axillae are operated at the same time. The use of locally available flaps on the lateral chest wall and medial side of arm is a very handy technique and has given consistently satisfactory results. References
Copyright 2006 - Indian Journal of Plastic Surgery The following images related to this document are available:Photo images[pl06005t1.jpg] [pl06005f3.jpg] [pl06005f2.jpg] [pl06005f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}