 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
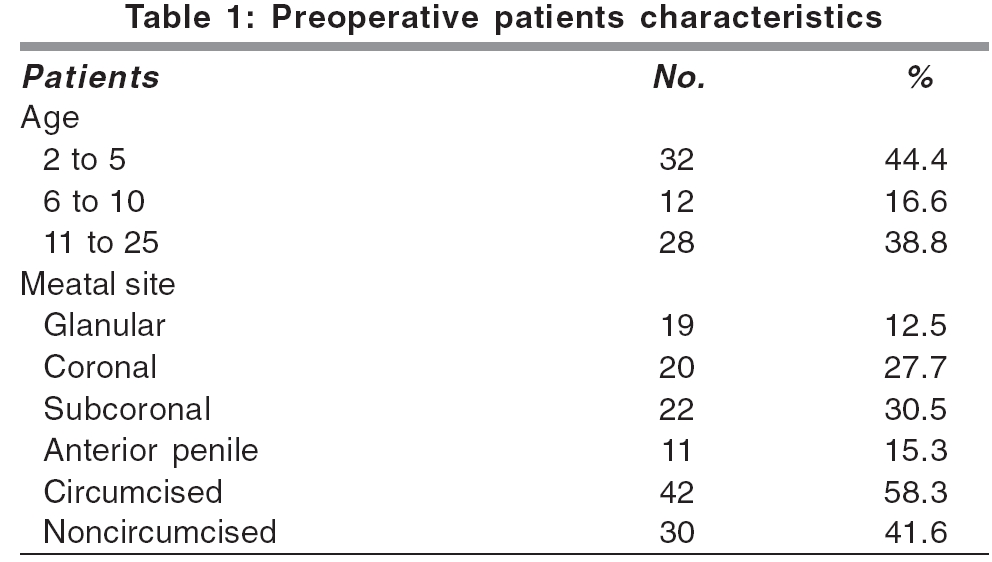
Indian Journal of Plastic Surgery, Vol. 39, No. 1, January-June, 2006, pp. 34-38 Original Article Urethral advancement technique for repair of distal penile hypospadias: A revisit Awad MohamedM.S Department of Plastic Surgery, Zagazig University, Zagazig Code Number: pl06008 Abstract Background: Numerous ingenious methods have been described to repair hypospadias with variable results. The anterior urethral advancement technique reported by Chang[1] to repair distal hypospadias has shown encouraging results. We have reevaluated this technique with some modifications to improve its results.Materials and Methods: This study was done on 72 patients, 19 cases with glanular hypospadias, 20 cases with coronal hypospadias, 22 cases of subcoronal hypospadias,and 11 cases with anterior penile hypospadias in the period between September 1999 and October 2003. The patients' age ranged from two years to twenty five years (median age 5.6) years. All the patients were operated using Chang's technique with our modifications. Results: There were no major complications in any of our patients, no postoperative fistulae or urethral stricture. Three patients had meatal stenosis and preputial edema occurred in 83.3% in non-circumcised patients. Conclusion: Modifications of the anterior advancement technique has produced excellent Results. It is easy to do and learn and also offers good cosmetic and functional results. Keywords: Advancement, hypospadias, urethra Introduction Any technique to repair distal hypospadias should be simple, easy and result in satisfactory functional and cosmetic outcomes, with few complications.[1] Many techniques have been described which relocate the urethral meatus and correct chordee. Ti Chang Shing[2] first described a technique in 1984, for treatment of distal hypospadias that meets these criteria with its unique character of avoiding anastomosis. This technique is associated with certain problems including difficulty for urethral dissection and postoperative meatal stenosis. Distal hypospadias represents the most common variant of hypospadias that the pediatric urologist treats.[3] Anterior urethral advancement is a technique for repair of distal penile hypospadias and urethral fistula by a one stage operation that can be used in circumcised and non circumcised patients with some drawbacks.[1] Thus, the aim of this study was to modify this technique to avoid these drawbacks.Materials and Methods Between September 1999 and October 2003 seventy two male patients with distal hypospadias were selected from the outpatient clinic of the Zagazig University hospitals. The patients were aged from two years to twenty five years (median age 5.6 years). In this series no=19 cases were of the glanular type, 20 patients had coronal hypospadias, 22 patients had subcoronal hypospadias while 11 had anterior penile hypospadias [Table - 1]. Forty two cases were circumcised, two of them had previously been operated and had developed postoperative anterior penile urethrocutaneous fistula, while thirty cases were non-circumcised. All patients were subjected to history taking, noting particularly history of previous operations, general and local examination of genitalia, bleeding and coagulation time. Surgical technique
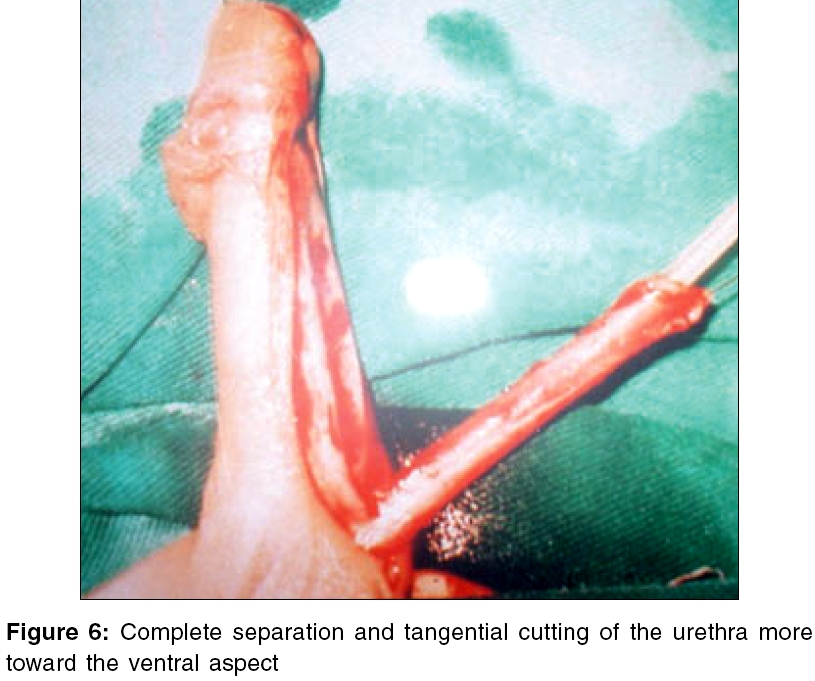
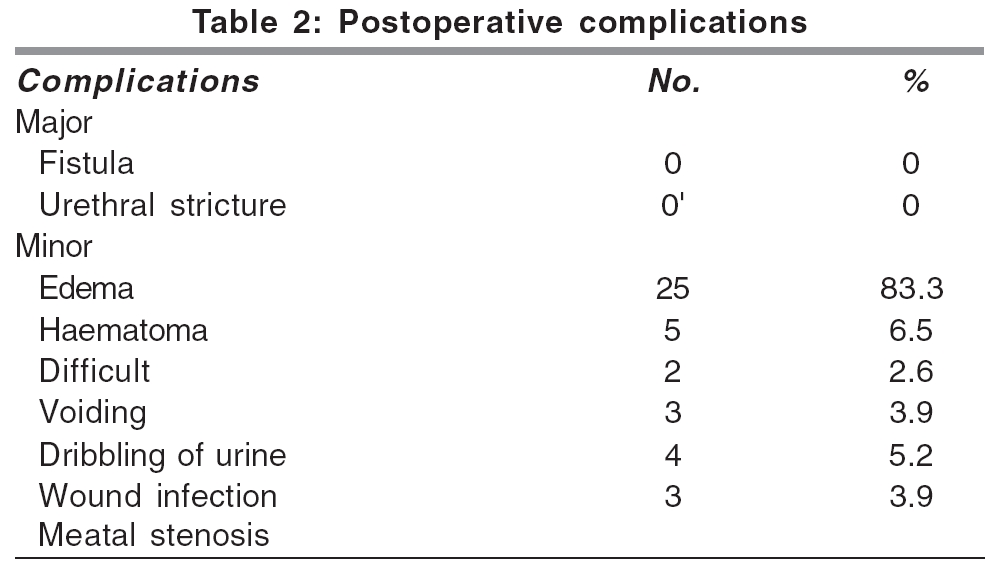
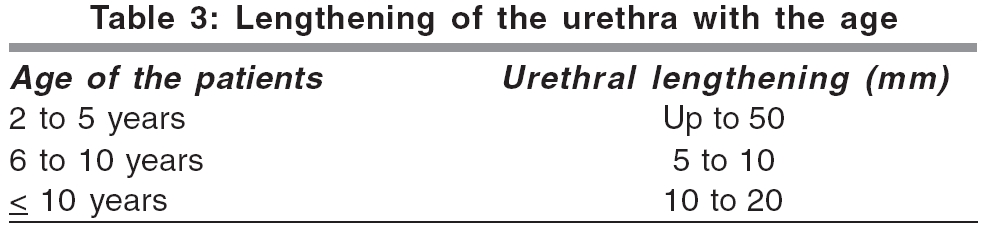
Results None of the patients had major complications, dehiscence, stricture or fistula. The most common minor complications were preputial edema (34.7%) not responding to any therapy [Table - 2] Problems immediately after surgery were rare; seventeen children (23.6%) had minor medical problems. Of these two had difficulty in voiding that was relieved with hot fomentation. Four patients had wound infection, five patients developed penile haematomas and three had significant meatal stenosis which was relieved with a dilator twice weekly for two weeks. At the review soon after repair the urinary stream was satisfactory in all but three children who had postvoid dribbling caused by crust and was relieved conservatively, Urethral elongation was an expected effect as shown in [Table - 3]. Discussion Management of patients with hypospadias usually requires sound surgical judgment to obtain optimal results and it is debated which technique should be used in specific anatomical situations.[4] In 1984, Ti Shing Chang[2] presented a technique for repairing distal hypospadias and urethral fistula by a one stage operation using the principle of advancement. The main drawbacks of this technique were meatal stenosis and the need for high degree of expertise in the surgeons to dissect the urethra without causing injury. In 1994 Elsaady[5] claimed that the cause of stenosis was inadequate opening of the glans for tunneling the urethra. He used the same technique with tunneling of the glans using hair transplant apparatus. This modification decreased incidence of meatal stenosis but was associated with another problem - that of decreasing the bulk of the glans leading to unsatisfactory cosmetic appearance. Using our modifications meatal stenosis was avoided in all patients by trimming the distal 2 mm of the urethra thus avoiding gangrene observed at the distal end, except in three cases (3.9%) where the stenosis was relieved by dilatation twice weekly in two weeks by passage of a catheter without anaesthesia. The time consumed to dissect the urethra until its tunneling and fixation to the glans ranged from 30 to 60 minutes with an average time of about 45 minutes. One more advantage over other procedures is that it does not need other tissues for covering the urethra. There is also no anastomosis between the urethra and the neo urethra, which can be a potential site for leakage and fistula formation. Further, the chordee (whatever its extent) has no influence on the procedure of advancement and can be corrected during the operation. All these factors contribute to the success of the TIP operation.[6] The extent of advancement of the urethra within its corpus can be estimated pre-operatively from as 0.5 to 2.5 cm, according to the age of the patients. In our study we noticed that the urethra can be advanced until 0.5 cm in patients with distal hypospadias aged from two to five years, about 1 cm in those aged from six to ten years and about 2.5 cm for those more than ten years. This observation agrees with the report of Koff[7] where the maximum length for urethral advancement was up to about 2.5 cm. Herberk et al[8] described the maximum length for urethral advancement of about 1.5 cm under optimal conditions in the preschool age. None of our patients developed postoperative fistula, meatal stenosis or urethral stricture as compared to the 0.5 to 10% incidence of fistula developing after a meatoplasty procedure[9] or 2.2 to 20% after the flip flap repair. [10] The incidence of fistula after tip operation has been described as 1% with a need for urethral dilatation by Elbakry.[11] Urethral stricture is the second most common major complication post hypospadias repair and the etiology depends on the type of repair and angulations of the anastomosis with or without distal obstructive complaints.[12] None of our patients developed urethral strictures as there was no anastomosis done and therefore no obstructive complaints occurred. Tunneling the glans through a vertical slit instead of a transverse slit gives a more or less normal appearance with good urinary stream [Figure - 9]. One of the observations we noticed while dissecting the urethra was that patients with large veins around the distal end of the urethra develop prolonged preputial edema in non circumcised patients. Most of the complications in our study were minor and acute and were treated conservatively in the hospital. All the patients voided normally with a good urinary stream.Conclusion Anterior urethral advancement technique with our modifications through the mobilisation of the urethra starting from its middle part and tangential cutting of the distal 2 mm of the urethra and vertical slitting of the glans is a simple technique. This method can be easily learnt, it is a rapid procedure giving the best cosmetic results with least complications. We prefer it to be done for repair of distal penile hypospadias as the best choice keeping in mind the relation between the patient age and the mobilized urethral distance needed.References
Copyright 2006 - Indian Journal of Plastic Surgery The following images related to this document are available:Photo images[pl06008f6.jpg] [pl06008f9.jpg] [pl06008t3.jpg] [pl06008f5.jpg] [pl06008f1.jpg] [pl06008f3.jpg] [pl06008f4.jpg] [pl06008t2.jpg] [pl06008t1.jpg] [pl06008f7.jpg] [pl06008f2.jpg] [pl06008f8.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}