 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
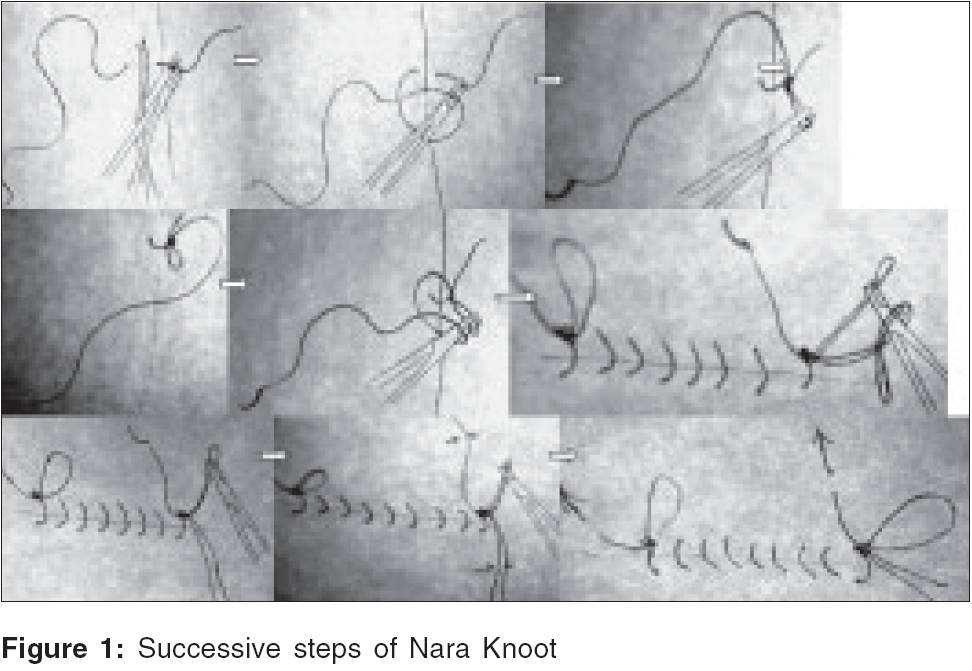
Indian Journal of Plastic Surgery, Vol. 39, No. 1, January-June, 2006, pp. 39-41 Original Article "Nara" knot for suturing of cleft lip in children to make removal easy Obaidullah, Aslam Mohammed Plastic Surgery Clinic, Aman Hospital, Dabgari Gardens, Peshawar - 25000 Code Number: pl06009 Abstract Cleft patients usually go through a lifetime of repeated hospital admissions and multiple procedures. Suture removal at a tender age and on a sensitive area like the lip becomes a challenge for the nursing staff. It is also emotionally demanding on the part of the parents. Hence, in most centres these patients are at least sedated if not anaesthetised. We have been using a simple knot and running prolene material so that undoing of the knot becomes easy and suture removal more or less atraumatic. We would like to share our experience with readers through this article. An analysis of 53 cleft lip repairs has shown that this knot is safe and easily removable. Keywords: Surgical Knot, suture knot, suture in children INTRODUCTION It has always been a difficult and emotionally challenging job to remove stitches in a pediatric population. Ideally, cleft lip repair is undertaken in early infancy. As the repair is undertaken under general anaesthesia, the cleft surgeon usually performs a delicate procedure using very fine sutures. Reports of skin repair with absorbable sutures[1] or surgical glue[2] are available but non-absorbable sutures are usually preferred for skin closure. However, removal of these stitches may be quite difficult with the crying baby and might be a cause of further distress to the family. Some stitches might be missed which have the potential of making a stitch abscess or leave a bad scar.[3],[4] Usually, the child is sedated. Sometimes, a short acting general anaesthetic is administered for removal of stitches. We perform surgery on new-borns and young children for various birth defects. Fine sutures are used, usually 6/0 prolene for skin closure. To obviate the need of sedation of the child and ease suture removal, we have been using a special knot and continuous suture for closure of skin wounds. The details of the stitch are illustrated. MATERIALS AND METHODS We retrieved records of all patients who had their cleft lip repaired under the age of two years from April 1st, 2004 to March 31st, 2005. Their notes were scrutinised for complications related to the suture technique. In all these patients we had used the special knot and running 6/0 prolene for skin closure. After approximating the muscles and mucosa with 5/0 vicryl and some subcutaneous stitches of 6/0 vicryl rapide are taken, skin closure is begun with the first stitch on the white roll of the vermilion. After taking a bite from both edges of the skin, a length of suture is left at the end. With the help of the needle holder, this length is grasped near the skin rather than at the end after throwing the first loop around the needle holder and a loop is pulled through the throw [[Figure - 1] and its subparts]. Pulling on the loop tightens the knot. This is secured by repeating one or more throws in the opposite direction but holding the loop to complete the square surgical knot. Further throws are put similarly if needed. It is exactly like tying shoe laces, leaving long loops on one side and free ends at the other. For opening the laces, all one needs to do is pull out the long hanging free end. This is the basis of our suturing technique with the only difference that suturing is completed by continuously running along the suture line. A similar knot completes the last stitch. Extra length of the double suture line and end is cut with scissors. There are redundant lengths of suture at both ends of the completed suture line. They are secured under carefully applied Steri-strips after painting the area with Tincutre Benzoin Co. [Figure - 2][Figure - 3]. The child is discharged home the next day. Parents are advised to keep the lip clean with the help of cotton buds and not to trim any suture material protruding. On the fifth to seventh postoperative day, the child is summoned to the outpatients. The child is not sedated but is steadied on the couch with the help of parents, under bright light. After cleaning the lip, Steri-strips are carefully removed. Sometimes the central two Steri-strips are left in place if the knots are exposed. The end of first stitch is clearly visible. It is grasped with a mosquito forceps [Figure - 1]. The child tries to move his/her head and the stitch unfolds itself with the slightest pull. The mosquito forceps is left attached to the suture. Similarly, the end of the last stitch is held with mosquito forceps and a little jerk from the child unfolds the last knot. Now Steri-strips are again applied after painting the skin with Tincture Benzoin Co. leaving the end of suture still in the mosquito forceps (if Steri-strips had been removed already). The end of the suture, which made the first knot, is pulled with the help of mosquito forceps. Prolene is very smooth and it easily slides out from the skin. Thus a three-step procedure completes the suture removal in a few minutes. [Figure - 4] shows a well healed lip. RESULTS A total of 53 patients were included in the study. Their ages ranged from 3 months to two years with a mean age of 6.3 months. There was a male to female ratio of 1.5: 1. The average period between the procedure and removal of stitches was 5.8 days. One patient fell at home on the second day of stitch removal and was hit on the wound resulting in partial disruption of the repair. He was taken to theatre for repair under general anaesthesia. Parents of three other patients trimmed the protruding ends. However, suture removal did not need sedation and we were able to remove them albeit with some struggling.DISCUSSION Suture removal in young children has been a difficult task both technically and emotionally. However, in most major surgical procedures, absorbable sutures have not taken the place of non-absorbable material though they are used to support subcutaneous tissue.[5] Because of the high price of synthetic early absorbable sutures. prolene is used. As a very fine suture of 6/0 Prolene, the knots are not bulky.[6] Hence, the search for the most atraumatic removal of stitches continues. With fine sutures like 6/0 Prolene and area of work on a sensitive site like the face, the task becomes even more difficult. Cleft lip (with or without palate) patients already put their parents through an emotional challenge and the situation worsens further during suture removal. With this background in mind, the authors have been using these knots for the last 10 years. We were a little surprised by the uniform use of sedation or even general anaesthetic for stitch removal by many colleagues in a recent symposium on clefts. When we suggested our knot, there was an almost unanimous concern about the safety of the knot. This was a risk we had, inadvertently, overlooked although we could not recall any premature un-doing of our knots. We therefore referred to the fact that this knot is very common in this part of the world where people wear baggy trousers. These trousers are not secured with any belt but with a woven cord. People universally use this knot for securing their trousers and they feel quite secure. This cord is known as "Nara", hence we named it as "Nara knot". As steri-strips make part of the support for the suture line, there is even less chance of suture line disruption.[4] In this study one patient had traumatic disruption of suture line one day later but this is not uncommon with other suturing techniques[7] and perhaps does not directly attribute the cause to the special knot. Besides other advantages, a running suture definitely takes less time than an interrupted suture line.[8]CONCLUSION The "Nara knot" is a safe means of securing a suture. Combined with over and over running technique, this makes suture removal easy especially in children with cleft lip repairs.References
Copyright 2006 - Indian Journal of Plastic Surgery The following images related to this document are available:Photo images[pl06009f2.jpg] [pl06009f1.jpg] [pl06009f3.jpg] [pl06009f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}