 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
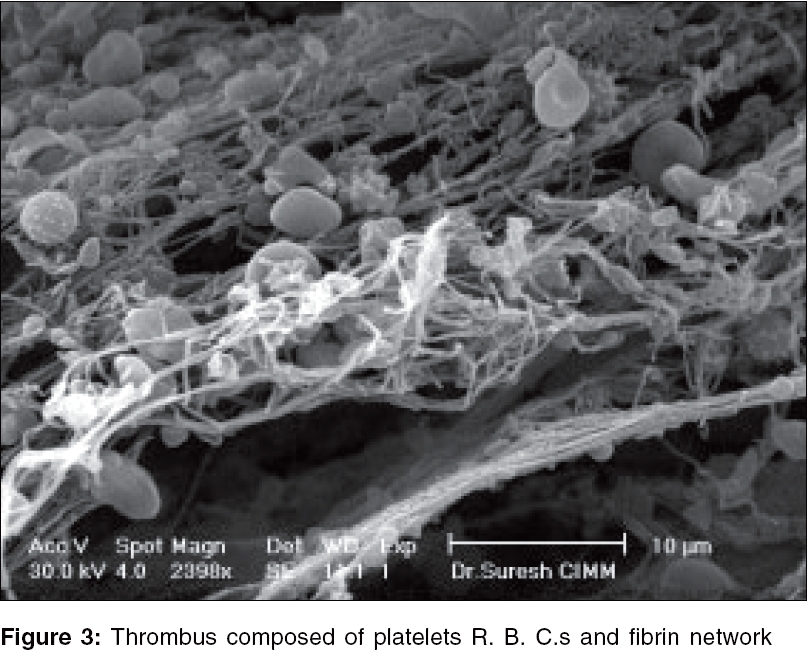
Indian Journal of Plastic Surgery, Vol. 39, No. 1, January-June, 2006, pp. 42-50 Original Article A scanning electron microscopic evaluation of microsurgical anastomosis by conventional end to end and end to end anastomosis using "temporary stent" technique: An experimental study Chaware SureshM, Bhatnagar SK, Singh AK Departments of Plastic and Reconstructive Surgery, King George's Medical University, Lucknow, U.P Code Number: pl06010 Abstract Background: The art of microvascular repair progressed slowly over a century after Carrel's original description of 'vascular repair' in 1902. Reports of the successful repair of vessels smaller than one mm in diameter are currently commonplace. However, the art of microvascular surgery has not yet been perfected, as evidenced by frequent reports of clinical failure. This study was undertaken to determine the effect of a 'temporary stent' on the patency rates of vessels and to study the vascular endothelium under electron microscope to determine the changes caused by both conventional and the experimental technique.Materials and Methods: This study consisted of two distinct arms. In the first part (27 rats) we studied the effect of temporary stenting on end to end anastomosis vis a vis its patency rates. While in the second part (30 rats) the same experiment was performed with a view to examine the anastomosis under electron microscope at different time frames to study the state of the endothelium in the vessel lumen at the site of anastomosis and also along the length of the vessel up to the point where clamps were applied. Results: In our study conventional end-to-end microvascular anastomoses had late patency rate of 70.37%. While end-to-end microvascular anastomoses using temporary stent had patency rate of 92.59%. On electron microscopic study, it was observed that, the endothelial damage was less in the stented group. Conclusion: Stent technique produces lesser degree of trauma to the vessel and no serious complications compared to the conventional dilatation and manipulation with vessel dilator. Keywords: Anastomoses, end to end temporary stent, microsurgical anastomosis INTRODUCTION The art of microvascular repair progressed slowly for last 100 years after Carrel's original description of a 'vascular repair'in 1902.[1] With refinement in the technique and instrumentation during the past five decades, the repair of severed blood vessels has now become a routine procedure. Reports of the successful repair of vessels smaller than one mm in diameter are commonplace. However, the art of microvascular surgery has not yet been perfected, as evidenced by frequent reports of clinical failure. Technical pitfall in the microsurgical anastomoses, such as intimal damage by forceps, inadvertent catching of the posterior wall, uneven placement of sutures and poor vessel wall apposition may all account for this lower patency rate. In this paper we present the "temporary stent" technique as a useful method of improving patency rates in the more difficult microsurgical anastomoses. We evaluated the anastomoses under electron microscope to study the various changes occurring at anastomotic site due to "temporary stent". MATERIALS AND METHODS This was an experimental study; healthy Swiss albino rats were taken for study having a weight of approximately 200 to 250 gms. Appropriate ethics committee permission was taken. This study was conducted on 27 rats for statistical analysis of patency and 30 Swiss albino rats for electron microscopic study and kept in an experimental laboratory during August 2003 to August 2004. All anastomosis were subjected to an evaluation at different time frames either for electron microscopy or for patency as described below: The 27 rats were divided in four groups, according period of observation i.e., 1st day, 4th day, 7th day, 14th day (In this group all anastomosis were patent at 15 minutes as observed on the operating table hence analyzing a 15 min. post operative set was of no significance). The 30 rats were divided in five groups of six each according to period of observation (15 min, 1 day, 4 day, 7 day, 14 day). Animals were anaesthetized prior to surgery with inhalation of ethyl ether initially and were maintained with ether anaesthesia by open method throughout surgery. All the anastomoses were performed by the same surgeon. Groins were shaved and cleaning of skin was done with betadine soaked sponge. The groin skin was incised along full length of groin fold. Femoral vessels were exposed in the femoral triangle. A piece of green background material was placed and clamps were applied over the artery. With the scissor at right angle to the vessel, the artery was transected with a single motion. Anastomosis was achieved with conventional "end to end" method on one side and the "temporary stent" technique on other side on the next day after the first anastomosis. This was done to avoid excessive blood loss and anaesthetic complications. The sides were reversed in consecutive rats. Suture material No. 10-0 nylon on round body 4 mm micro point needle was used as suture material in all the anastomoses. Microanastomosis by temporary stent technique In the "Temporary stent" technique group, no dilation of the vessel with vessel dilator was permitted, since the idea was to study the effect of stent and vessel dilator on intimal surface and effect on patency. Two corner stitches, 180 degree apart were inserted and tied [Sketch 1]. A short segment (2-3 mm) of nylon suture (6-0) was then inserted through both divided ends into the lumen of the vessel and kept there as a stent whilst the anastomosis was being performed [Sketch 2]. Three to four evenly spaced stitches completed the anterior wall repair [Sketch 3]. The vessels were turned over to expose the posterior wall and another three to four stitches were evenly inserted and kept long and untied [Sketch 4]. This stent was gently removed with forceps [Sketch 5] and the sutures were then tied one by one [Sketch 6]. Eight to ten stitches were sufficient for all anastomoses using the "temporary stent" technique. However, in the "conventional method" group, occasionally one or two more stitches were needed to complete the repair and prevent significant leak. This was because of unevenly spaced sutures. The distal clamp was removed first and back filling across suture line was noted. After that the proximal clamp was removed. The distal pulsation was noted. Flicker test was done. After 15 minutes milking test was done. Photographic documentation was done during and after completion of the anastomosis. Vessel assesment In the first arm of the experiment, to study difference if any, in patency rates, the 27 rats were divided in four groups, according to period of observation viz. 1 day, 4 days, 7 days, 14 days for statistical analysis and re-exploration was done on the particular day to confirm the patency. The rats were subsequently sacrificed using humane permitted methods. In the second arm of the experiment, post anastomotic follow up study was done in five groups for electron microscopic examination. In each group rats were kept under observation after anastomoses. In first group each anastomosis site was checked for patency after 15 minutes. Biopsy was taken of the anastomotic site from both groins after ligating vessels at proximal and distal end. In second group rats were observed for 24 hours duration and reexploration for patency and biopsy was done. Same procedure was done in rats of third group after four days, in fourth and fifth group after seven and fourteen days respectively. The rats were subsequently sacrificed using humane permitted methods. Preparation for scanning electron microscopic study At selected time interval after anastomosis (15 minutes, 24 hour, 4th day, 7th day and 14th day) each group containing 6 rats was re anesthetized. Vessel patency was tested under the operating microscope using the downstream squeeze test. Via the abdominal aorta, the vessels were fixed by a 15 minutes perfusion with a 1:3 dilution of the Karnovsky's fixative, consisting of 1.0% paraformaldehyde plus 2.5% glutaraldehyde in 0.1M sodium cacodylate buffer, pH7.3. The anastomotic segments about 1cm on either side including the area under the vascular clamps were removed and fixation was continued for at least 24 hours by immersion in Karnovsky's fixative, consisting of 1.0% paraformaldehyde plus 2.5% glutaraldehyde in 0.1 M sodium cacodylate buffer, pH7.3.The vessels were dried with graded ethanol upto critical point. Vessels split longitudinally in two segments, mounted on aluminum stubs, coated with gold. Specimens were studied in an ESEM XL-30 scanning electron microscope. RESULTS The patency rates of end-to-end anastomoses by conventional technique [Table - 1] The total patency rates of conventional end-to-end anastomosis were 19/27 (70.37%)FNx01. FNx01Corrected value includes two cases where posterior wall was caught during the anastomoses. Anastomoses were resected and redone and hence not considered patent. The patency rates of end-to-end anastomoses using temporary stent [Table - 2] The total patency rates of end-to-end anastomoses using temporary stent were 25/27 (92.59%). This difference was statistically significant ( P < 0.001), (Chi-square test). A scanning electron microscopic study on operated artery [Figure - 1] The luminal surface was nearly smooth, with some longitudinal corrugation that seems to undulate and run in a gentle spiral. This corrugation corresponds to the ridges in the internal elastic lamina; they are very prominent in vessels in spasm. The luminal surface is covered by a single unbroken layer of endothelial cells in which the cell borders are not usually discernible without special stains. Microvilli, platelets, red blood cells are occasionally seen. Fibrin and leukocytes are never seen adhering to the undamaged endothelium. Group 1: 15 minutes after anastomosis The effect of the surgical repair on the vessel wall was assessed 15 minutes after the operation when the anastomotic site was least likely to be obscured by thrombus. 6 arteries by conventional method of anastomosis and 6 arteries by temporary stent technique of anastomosis were examined at this time interval. Conventional end to end anastomosis Arteries showed severe tearing and desquamation of the endothelial sheet associated with vessel dilation with metal vessel dilator and the suture and deposition of the thrombus over the anastomotic site. Apposition of the cut edges was tighter but overlapping was uncommon. A gathering of the vessel wall beneath the suture was invariably present and poor axial alignment of the vessel ends resulting in longitudinal corrugation in the wall occurred in 3 specimens to some degree. Suture tension, a critical factor in the survival of the anastomosis, particularly in the arterial repair, could be assessed by observing the degree of curvature of the thread projecting into the lumen. When tied too tightly the sutures appeared flattened. But because of deposition of the thrombus over the anastomotic site very few sutures were visible. Thrombus extended over the suture and the luminal surface, the area covered and the degree of resultant luminal reduction were variable. Luminal reduction of moderate degree was observed in 2 specimen and one specimen showed minor reduction. Red cells plugged the needle holes and the gap between the cut ends. The thin mural thrombus consisted of high proportion platelets with red cell and fibrin, thrombi that projected in the lumen had a greater proportion of red blood cells. Area between anastomotic site and clamp site The endothelium showed widespread loss of surface detail and widespread areas of endothelial desquamation. Sharp defined area of endothelial loss occurred close to the anastomotic site. This type of injury appeared to result from the technique of mechanically dilating the artery with forceps. Thrombus formation at this site was similar to that noted at clamp injury site. Luminal surface of vessel was covered with variable proportion of scattered adherent blood cells and layer of mural thrombus. Both type of deposit consisted mostly of platelets and red cells. End to end anastomosis using temporary stent Arteries showed less desquamation and tearing of the endothelial sheet associated with use of temporary stent of nylon and less deposition of the thrombus over the anastomotic site. Apposition of the cut edges appeared to be under adequate tension without overlapping of the edges. A gathering of the vessel wall beneath the suture was present but less than conventional group. Suture was placed more regularly. Suture tension, assessed by observing the degree of curvature of the thread projecting into the lumen. When tied to tightly the sutures appear flattened. It was observed that suture tension was adequate. Thrombus extended over the suture and the luminal surface, the area covered and the degree of resultant luminal reduction were less compared to the conventional group. Red cells plugged the needle holes and the gap between the cut ends. The thin mural thrombus consisted of high proportion of platelets with red cell and fibrin. Area between anastomotic site and clamp site The endothelium showed patchy loss of surface detail and focal areas of endothelial desquamation. This was in contrast to the sharp defined area of endothelial loss which occurred close to the anastomotic site in conventional group. In the temporary stent group, mechanical dilation of the vessel was not done with a vessel dilator. Thrombus formation at this site was focal and minimal to that noted in conventional group. Luminal surface of the vessel was covered with a variable proportion of scattered adherent blood cells and a layer of mural thrombus. Both type of deposit consisted mostly of platelets and red cells. Group 2: 24 hours after anastomosis Anastomotic site On the endothelial surface, numerous platelets forming dendritic processes at the suture site were found. The amount of platelets and fibrin was higher close to the site of the break, at the needle insertions. On the rest of the suture material in the lumen, only a few platelets could been seen. Endothelial injury seen as loss of surface detail of cells or desquamation of the endothelial sheet. This may be due to leukocytes migration. Platelets contributing to the thrombus were seen in various forms. An activated form with numerous cytoplasmic projections from the surface was common but mostly they were seen as spread stellate shape, sometime reaching a diameter of 7 µm. These spread platelets appeared to be inactive, forming a non-thrombogenic temporary pseudo-intima. Area between anastomotic and clamp site The luminal surface was covered with a combination of thin layer thrombus, scattered blood elements and occasionally obstructing thrombus. The density of these deposits decreased with distance from the anastomosis. Platelets and leucocytes were the most common cells present; fibrin was rarely seen. No endothelial regeneration was present. Group 3: 4 day after anastomosis Anastomotic site Cells that resembled monocytes or small macrophages were found on the sutures. These cells had a minimum diameter of approximately 12 µm. Larger cells more closely resembling macrophages were also present. Area between anastomotic and clamp site There was a combination of loss of thrombus and regeneration of endothelium. Single cells or group of cells densely covered with microvilli and resembling cells at the growing edge of the endothelial sheet could be seen among the thrombus. Group 4: 7 days after anastomosis Anastomotic site Regeneration of the endothelium had begun. The suture was covered either with a fibrinous mesh or with newly formed endothelial cells. There was a carpet of endothelial cells with clearly demarcated intercellular junction reaching almost to the suture line. The sutures appeared coated with amorphous material. Area between anastomotic and clamp site Group 5: 14 daysafter anastomosis Re-endothelisation was virtually completed by two weeks, sutures were almost or completely covered and clamp injuries were no longer visible. The endothelial cells were irregular in outline and not flow oriented. DISCUSSION The needle and thread are still used for vascular anastomosis, more or less as described 100 years ago. Although fine sutures have provided the basis of microsurgical technique since its inception, the suture technique is limited by the size of the vessel under study. The smaller the vessel, the greater the percentage of stenosis and deformity caused by the sutures. Although the change in luminal diameter of a repaired human aorta may be imperceptible, each suture in the repair of a 0.5 mm vessel slightly reduces the vessel's diameter, no matter how well the anastomosis is performed (Moskovitz et al .).[2] Technical pitfalls in microsurgical anastomosis such as intimal damage by forceps, inadvertent catching of the posterior wall, uneven suture spacing and poor vessel wall apposition may all account for lower patency rate. Use of a temporary stent may obviate this problem. (Wei et al . 1982)[3] In the "temporary stent" technique we used 2-3 mm piece of nylon 6-0 as stent, which is readily available. Wei, Mancer and Juker,[3] used short segment (3-4 mm) of medical grade silastic tube as a temporary stent. In our study the conventional end-to-end microvascular anastomoses had 77.77% patency rate and end-to-end microvascular anastomosis using temporary stent technique had patency rate of 92.59%. Further, in the "conventional technique" group, in two rats, posterior wall was caught during anastomosis. Resection and redo of anastomosis was done. Considering this as failure, total patency rates in the conventional group were 70.37%. (19/27) This difference is statistically significant ( P < 0.001) (Chi-square test) In the non-operated control vessel, the ridges seen in the lumen of arteries result from the folding of internal elastic lamina due to contraction of the underlying smooth muscle and are a normal physiological occurance.[4] The function of these convolutions is unclear, but it would appear that they reduce turbulent blood flow.[5] Scanning electron microscopic study of the luminal surface of the arterial specimen shows that striking differences were observed during the initial period of anastomosis. In the conventional group, it was observed that, there was extensive damage to the endothelial sheet associated with use of metal vessel dilator leading to deposition of extensive thrombus. Nightingale et al .[6] reported, surgical manipulation results in damage to the smooth non-thrombogenic surface of the vessel. They stated that the three potential sources of reduced patency associated with the anastomotic site were
The last two factors could be more severe if combined with an excessively large bite and / or excessive suture tension. We observed that temporary stent causes
Late changes, such as inflammation, endothelial cell migration and re-endotheliliazation were almost same in both groups. A study of literature showed no references showing effects of stent on endothelium CONCLUSION We conclude that 'temporary stent' can effectively prevent the damage to the endothelium. If an anastomosis is to be performed by a micro surgeon who is less skilled in the manipulation of very small vessels the results might well be better with 'temporary stent' technique.ACKNOWLEDGEMENTS I am forever indebted to Dr. V. K. Bajpai, Scientist, and In-charge, Electron Microscopy Laboratory, Central Drug Research Institute, Lucknow for extending his help at all those innumerable times when I required it the most and especially in scanning electron microscopic analysis. His hand of help always reached out for me and oriented me over so well. He has been an incessant source of illumination for me. His scholarly advice reaped me great asset to accomplish this study.References
Copyright 2006 - Indian Journal of Plastic Surgery The following images related to this document are available:Photo images[pl06010f8.jpg] [pl06010f4.jpg] [pl06010f20.jpg] [pl06010f16.jpg] [pl06010f5.jpg] [pl06010f12.jpg] [pl06010f14.jpg] [pl06010f3.jpg] [pl06010f7.jpg] [pl06010t2.jpg] [pl06010f21.jpg] [pl06010f2.jpg] [pl06010f13.jpg] [pl06010t1.jpg] [pl06010f18.jpg] [pl06010f19.jpg] [pl06010f9.jpg] [pl06010f17.jpg] [pl06010f6.jpg] [pl06010f15.jpg] [pl06010f11.jpg] [pl06010f1.jpg] [pl06010f10.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}