 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
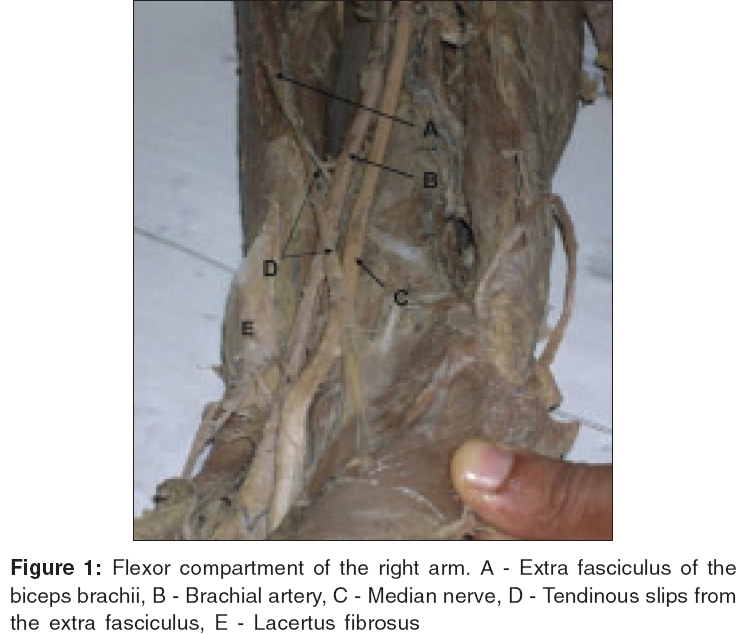
Indian Journal of Plastic Surgery, Vol. 39, No. 1, January-June, 2006, pp. 65-67 Case Report A rare variation of the biceps brachi muscle Paval J, Mathew JG Department of Anatomy, Melaka Manipal Medical College, Manipal - 576 104, Karnataka Code Number: pl06014 Abstract Biceps brachii muscle is very variable. Biceps may be composed of one to five heads. Although the variations in the origin are plenty, there are a very few cases reported on the variations in the insertion of the biceps brachii muscle. In this report we present a variant biceps brachii muscle which gives an abnormal muscle fasciculus from its medial side which continues as a narrow tendinous slip and is inserted in to the medial supracondylar ridge of humerus. We discuss in this report, the possible median nerve entrapment due to the presence of such a variation.Keywords: Biceps brachii, brachial artery, median nerve Introduction The most studied and reported upper extremity nerve entrapment problem is those related with the median nerve. Among these, the most common one is the carpal tunnel syndrome. Because this condition is studied so often, clinicians may be too eager to assume the presence of carpal tunnel syndrome for any kind of median nerve compressions. In this report we discuss a possible median nerve entrapment in the cubital fossa by an abnormal tendinous slip from the biceps brachii muscle.Case report During the routine dissection for medical students, we found an abnormal insertion of biceps brachii muscle unilaterally in a male cadaver. The origin of this biceps brachii was normal. The muscle followed a normal course and most of the muscle fibres formed a round tendon and was inserted to the radial tuberosity of radius. But some of the fibres from the medial side below the level of the middle of the arm formed a separate muscle bundle and continued as a narrow tendinous slip [Figure - 1]. This slip soon divided into two- the lateral slip was found superficial to brachial artery and median nerve and the medial slip was deep to them. The lateral slip crossed the cubital fossa, merged with the fascial covering of the flexor carpi ulnaris muscle. The medial slip curved medially and was attached to the medial supra-condylar ridge of the humerus.Discussion The important variations of biceps brachii reported by Macalister are as follows;[1]
1. The muscle may be entirely suppressed A separate slip from coracobrachialis continuous with the short head is described by Wood and Macalister. They also described a doubled coracoid head and this anomalous portion may join the main body of the muscle or else it may unite with the normal coracoid head before that portion of the biceps joins the long head.[1],[2] Mori described various origins of the third or accessory head as follows: In 50 arms there were 10 (20%) arms with a third head of the biceps.[3] The origins of these additional heads were: 1. The distal portion of the deltoid tuberosity, 4 arms, 8%. The two other accessory heads are rare and take several different forms. When fully developed, they arise close together from the neck of the humerus, below the lesser tubercle and behind the pectoral tendon to which they may be more or less joined. The more lateral of the two slips joins the long head of the muscle, whereas the medial joins the short head.[3] In other instances (Spinner et al ), the two heads of the biceps muscle may be totally separate or fused and either head may be absent. In the absence of the long head, the tendon may be found arising from the bicipital groove, one of the tubercles, the capsule of the joint or the tendon of pectoralis major. The tendon may be doubled or it may be represented only by the aponeurosis.[4] The aponeurosis or the lacertus fibrosus which may be doubled may compress the median nerve as found in the pronator syndrome.[5] The pronator syndrome was first described in 1951 by Seyffarth.[6] He reported 17 patients whom he proposed were suffering from median nerve entrapment as the nerve passed through the pronator teres muscle or the flexor digitorum superficialis (FDS) arch. This illustrates that from the time of the initial description, there has been ambiguity about the name because it includes more than just compression by the pronator teres. It is now often referred to as the so-called pronator syndrome because it has a common clinical presentation but a "spectrum" of locations of compression. Since 1951, there have been numerous reports of patients presenting with pronator syndrome who have gone on to surgical decompression with complete recovery. There are four more commonly described locations of compression: 1. Ligament of Struthers-an uncommon structure that is rarely believed
to cause pronator syndrome.[7],[8] The most common areas of compression of the median nerve are at the level of the FDS arch[12] or by the nerve passing through the pronator teres muscle.[13] In the present case, biceps brachii had an accessory muscle fasciculus and this continued as a tendinous slip. This variation is different from the cases of doubling of lacertus fibrosus. Looking at the close relationship with the median nerve, this variation can also be considered as one of the potential cause of the pronator syndrome. The pronator syndrome is much less common than the carpal tunnel syndrome (CTS). It usually presents in the fifth decade and is four times more common in women.[13] The symptoms are insidious in onset, with a delay in diagnosis ranging from 9 months to 2 years.[8],[12],[15] The patient most commonly complains of aching pain in the proximal forearm and the distal arm. Pain may radiate proximally and is often aggravated by use of the upper limb, especially with resisted forceful pronation or repeated pronation/supination movements.[5],[6] As is the case in CTS, there is usually associated paresthesiae and, possibly, altered sensibility in the radial three and a half digits,[8] but night awakenings and nocturnal pain are uncommon- a key symptom to help differentiate from CTS. The differential diagnosis of the pronator syndrome is extremely important because this entity is relatively uncommon compared with CTS. In fact, as noted by Lister,[5] Symptoms of CTS are very similar to those of pronator syndrome.[5] Similarities between two syndromes:[5] Pain in wrist and forearm regions, weakness of thenar muscles numbness/paresthesias of radial three and a half digits. Differences in two syndromes:[5] No nocturnal pain in pronator syndrome, negative Tinel's sign at wrist in pronator syndrome, nerve conduction study shows - no delay at wrist in pronator syndrome. Dysesthesia in palmar cutaneous distribution is seen in pronator syndrome. Other important differential diagnosis include thoracic outlet syndrome, proximal brachial plexus neuropathies, cervical radiculopathy and polyneuropathy. The diagnosis of these conditions is assisted by the use of electrophysiologic investigations.[5] Considering the entire length of the median nerve, there are numerous locations that median nerve entrapment may occur. It is very much essential to thoroughly evaluate the problem before coming to a conclusion about the presence of the popular compressive neuropathies. References
Copyright 2006 - Indian Journal of Plastic Surgery The following images related to this document are available:Photo images[pl06014f1.jpg] |
| |||||||||

{kind=link}