 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
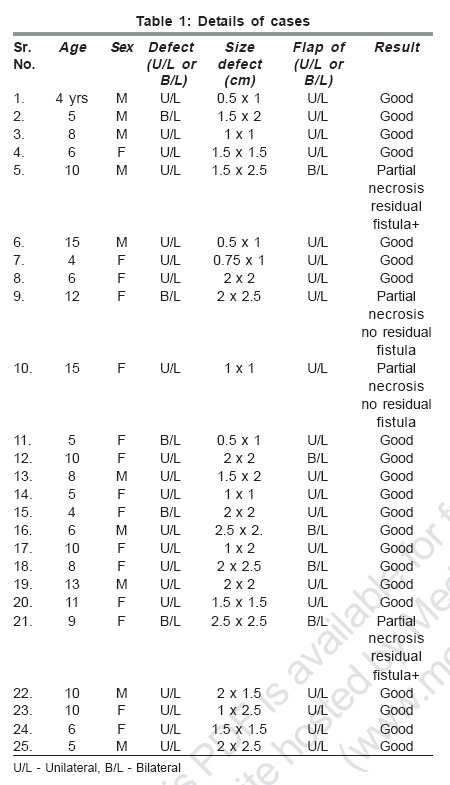
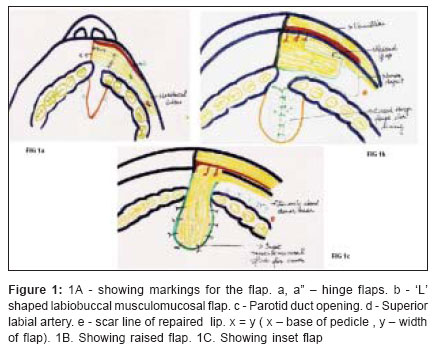
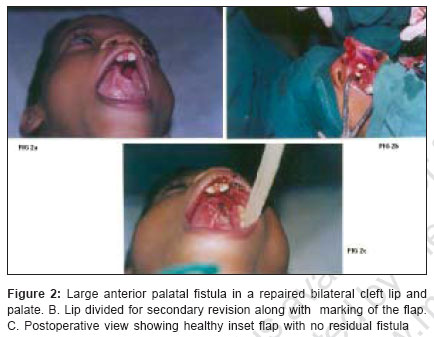
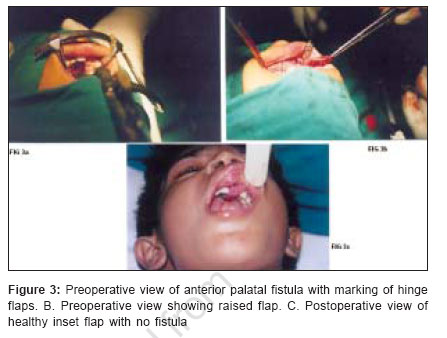
Indian Journal of Plastic Surgery, Vol. 39, No. 2, July-December, 2006, pp. 148-151 Original Article Orbicularis oris musculomucosal flap for anterior palatal fistula Tiwari VK, Sarabahi Sujata Department of Burns and Plastic Surgery, Safdarjung Hospital, New Delhi Code Number: pl06036 Abstract Anterior palatal fistulae or residual anterior clefts are a frequent problem following palatoplasty. Various techniques have been used to repair such fistulae, each having its own advantages and disadvantages. We have successfully used orbicularis oris musculomucosal flap to close anterior fistula and residual clefts in 25 patients. This study shows the superiority of this flap over other techniques because of its reliable blood supply, easy elevation and transfer to fistula site and finally because it is a single-stage procedure.Keywords: Labiobuccal sulcus, musculomucosal flap, palatal fistula Introduction The most common complication following palatoplasty is a fistula or a residual cleft in the anterior palate. Fistulae occur more frequently after repair of a complete cleft of the primary and secondary palate than after isolated secondary palate repair. The main reasons for anterior palatal fistula are inadequate anterior repair at primary surgery of the lip in a complete cleft, infection, hematoma, excess tension on repair or flap necrosis. Fistulae can be large or small. Small defects can be ignored but large defects cause significant functional problem in speech and nasal regurgitation of food and fluids and therefore have to be repaired early. There is considerable scarring in the palate after palatoplasty because of raising of mucoperiosteal flaps. Hence, even though local palatal flaps can be used to close the fistula, the mucoperiosteum which is stiff and scarred by previous procedures, is difficult to transpose. Also, it will further increase the scar tissue which causes deformities in the maxillary arch because of its contracture. Therefore, labiobuccal flap, which includes the orbicularis oris muscle along with the mucosa, being a regional flap is a better alternative to local palatal tissue for repair of these fistulae. It is a safer flap because of its well-defined blood supply. The advantage of including the muscle with the mucosa is that in all such cases the lip has also been operated upon so there is a scar line in the lip and buccal sulcus. So if the mucosa is raised alone then only a small random pattern flap can be raised. Since muscle is included along with mucosa, the superior labial artery along with its branches is included in the flap base. As these branches supply the muscle, a longer flap can be raised, which increases its reach till the anterior two-thirds of the hard palate. It can also be combined with bone grafting because of the extra vascularity provided by the muscle. Materials and methods We have operated on 25 patients [Table - 1], of which 10 were male and 15 were female aged 5 to 15 years. Of these, 20 patients had undergone a primary push back palatoplasty using mucoperiosteal flaps for unilateral complete clefts of the primary and secondary palate (Group III Ritche -Davis) and five patients had undergone the same for bilateral complete clefts. Fifteen patients had already undergone a previous repair for anterior fistula using some local palatal tissue and hence had excessively scarred palate. The width of the fistulae varied from 0.5 to 1.5 cm and length varied from 0.5 to 2.5 cm. Anatomy of the flap [Figure - 1]A-C The superior labial artery on the lateral side of the cleft lip follows the course of the orbicularis muscle bundles and the edge of the cleft upwards to the nasal ala where it anastamoses with the lateral nasal or angular artery. The flap is raised from the labiobuccal sulcus based superiorly proximal to the scar line of the operated lip. Inferiorly, the scar line is included as the margin of the flap, making it a ′L′ shaped flap. Hence the flap is based on the branches of the superior labial artery (which runs along the vermilion of the repaired lateral segment) which are given off proximal to its terminal end which had been ligated or cauterized during lip repair. A good chunk of the orbicularis oris muscle included in the flap is supplied by these branches thus making it a myomucosal flap. Operative procedure The nasal lining in all cases was provided by raising hinge flaps a - a" [Figure - 1] from the margins of the defect. Following this the actual defect for which the oral lining cover was required could be assessed. Of the 25 patients, a unilateral labiobuccal musculomucosal flap was raised in 20 patients from the same side as the cleft and bilateral flaps were raised in five patients in whom the defect was larger. Everting the lip and cheek, the parotid duct opening was localized. Then the flap was marked and raised including the mucosa and the underlying orbicularis oris muscle till the periosteum. The distal most end of the flap can extend till the parotid duct opening depending on the length of the flap required [Figure - 1]A. The superior margin of the flap runs 3 mm above the gingival margin and extends till the scar line of the repaired lip. The inferior margin stops before the scar line at a distance ′X′ which is equal to the width of the flap ′Y′, thus raising an ′L′ shaped flap based on the superior labial artery which runs in the margin of the vermilion. The donor defect was closed primarily by interrupted sutures. This flap was then transposed through the cleft in the alveolar arch to the fistula and sutured to the margins of the oral lining of the palate around the fistula to provide cover over the hinge flap [Figure - 1]C. In four cases the alveolar arch had no visible cleft with all teeth in position. As a result the flap pedicle passed over the lateral incisor / canine tooth and was likely to be bitten off between occluded teeth postoperatively. Therefore, a plastic protector was made and placed over the dentition at the end of operation to protect the pedicle. In five cases the residual cleft was large and midline in position and single flap was insufficient to cover the defect. In these cases, bilateral orbicularis oris musculomucosal flaps were raised and transposed to completely cover the defect. In two cases the procedure was combined with secondary revision of the lip of same side. This was largely a single-stage procedure and did not need division of the pedicle as it passed through the cleft in the arch, except in the four cases in which the flap passed over the permanent dentition. Result [Table - 1]The flap healed without any complication in 21 cases [Figure - 2][Figure - 3]. In four cases in whom the dentition impinged upon the pedicle of the flap, the flap was partially lost as the bite block could not be maintained as these patients were all children. However, the hinge flap provided adequate cover to the fistula and there was no residual defect in two cases. In the remaining two cases there was a residual fistula which needed a secondary repair at a later stage. Discussion Anterior palatal fistulae have been closed by conventional methods by various surgeons using local, regional or distant tissue.[1] Most often either hinge flaps alone or along with local advancement flap, rotation flap[2] or palatal island flap[3] are used for small fistulas. Lehmann[4] used Veau flaps with buccal mucosal flap for fistula closure along with bone graft to fill bony defect. Herbert[5] used bilateral mucoperiosteal island flap as lining and cover both, for middle third fistulas in unscarred palate. But in postpalatoplasty cases with large fistulas, local mucoperiosteal flaps cannot move much because of severe fibrosis and scarring from primary surgery. Furthermore, if palatal mucosa is again widely mobilized and raised, there is more scar contracture which hampers maxillary growth and causes arch deformities also. For such cases regional tissue or distant tube pedicle flaps from the arm or abdomen[6],[7] were considered to be a better option. Large palatal fistulae were first shown to be successfully managed by tongue flap by Guerro-Santos and Altamirano[8] and later by Pigott et al , Qattan, Guzel et al .[9],[10],[11] and many other authors. However, it has the disadvantage of being a two-stage procedure with anticipated intubation and extubation difficulties, risk of flap separation because of tongue movement, aesthetically unpleasant bulky tissue, postoperative tongue deformity with articulation defects. In the past two decades, the buccal mucosa with buccinator muscle has also been widely used for cleft palate repair[12] and for palatal fistula repair.[13] Though it has a reliable blood supply with no donor site morbidity, it is a two-stage procedure. It was useful mainly for fistulae in the middle third and posterior third of the palate and unreliable for anterior hard palate fistulae. Rintala[14] used the labiobuccal mucosal island flap with hinge flaps for anterior fistulae and residual clefts but since it was a random mucosal flap with no specific vascular supply its length was limited. Another random pattern buccal mucous membrane flap from gingivobuccal sulcus has been used by Hirshowitz and Mahler[15] for alveolar clefts where canine and first molar tooth are missing. The principal advantages of our orbicularis oris musculomucosal flap are as follows:
The only limitation of our flap is seen in cases where the entire dentition is intact with no cleft in the alveolar arch because of which the flap pedicle runs over the teeth and is likely to be bitten off if a bite block is not maintained properly postoperatively. References
Copyright 2006 - Indian Journal of Plastic Surgery The following images related to this document are available:Photo images[pl06036f1.jpg] [pl06036t1.jpg] [pl06036f3.jpg] [pl06036f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}