 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
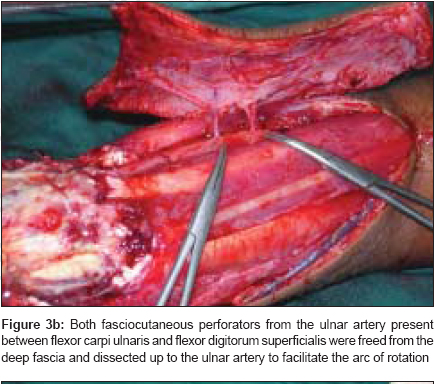
Indian Journal of Plastic Surgery, Vol. 40, No. 1, January-June, 2007, pp. 12-17 Original Article The distally-based island ulnar artery perforator flap for wrist defects Durga Karki, A. K. Singh Post Graduate Department of Plastic and Reconstructive Surgery, King George Medical University, Lucknow, Uttar Pradesh Code Number: pl07006 Abstract Background: Reconstruction of soft tissue defects around the wrist with exposed tendons, joints, nerves and bone represents a challenge to plastic surgeons, and such defects necessitate flap coverage to preserve hand functions and to protect its vital structures. We evaluated the use of a distally-based island ulnar artery perforator flap in patients with volar soft tissue defects around the wrist.Materials and Methods: Between June 2004 and June 2006, seven patients of soft tissue defects on the volar aspect of the wrist underwent distally-based island ulnar artery perforator flap. Out of seven patients, five were male and two patients were female. This flap was used in the reconstruction of the post road traffic accident defects in four patients and post electric burn defects in three patients. Flap was raised on one or two perforators and was rotated to 180º. Results: All flaps survived completely. Donor sites were closed primarily without donor site morbidity. Conclusion: The distally-based island Ulnar artery perforator flap is convenient, reliable, easy to manage and is a single-stage technique for reconstructing soft tissue defects of the volar aspect of the wrist. Early use of this flap allows preservation of vital structures, decreases morbidity and allows for early rehabilitation. Keywords: Island flap, ulnar artery perforators, wrist defects Reconstruction of soft tissue defects of the wrist with exposed tendons, nerves, joints and bone represents a challenge to plastic surgeons, and such defects necessitate flap coverage to preserve hand functions and to protect its vital structures. There are very limited options for flaps to cover them, especially so in volar wrist defects. When underlying structures are exposed, the split skin graft has a limited role, the need for flap cover can be met either by a local flap, distant flap or free flap. The field of reconstructive surgery has taken a significant leap forward with the introduction of perforator flaps. The primary advantage of perforator flaps is the minimization of donor site morbidity. Perforator-based surgery has added a new dimension to the field of reconstructive surgery. We describe the use of the distally-based island Ulnar artery perforator flap for volar wrist defects and present our results. The distally-based forearm island flap is vascularized by the fasciocutaneous perforators of the Ulnar artery. It fulfils all the necessary criteria for a flap providing thin pliable healthy hairless skin Anatomy The brachial artery divides into radial and ulnar arteries one cm below the elbow joint. The ulnar artery gives off anterior and posterior ulnar recurrent arteries and passes deep to pronator teres where it gives off the common interosseous artery. It continues toward the medial side of the forearm where it lies beneath the flexor carpi ulnaris on top of the flexor digitorum profundus. The anterior and posterior Ulnar recurrent arteries give off small branches to the skin respectively in front of and behind the elbow. The remainder of the ulnar territory is supplied by a series of about five or six perforators which reach the surface by passing along the fascial septum between the flexor carpi ulnaris and Flexor digitorum superficialis. Generally these perforators pass in front of the ulnar nerve. Their branches tend to fan out in all directions rather than being mainly transversely oriented [Figure - 1]. Materials and Methods Between June 2004 and June 2006, seven patients of soft tissue defects on the volar aspect of the wrist underwent distally-based island Ulnar artery perforator flap. Five patients were male and two patients were female, ages ranging from 22 to 50 years (mean, 31.8 years), and follow-up ranging from four to 24 months (mean, nine months). They comprised four cases of electrical burn injury and three cases of crush injury in road traffic accidents (RTA). The sizes of the flap ranged from 5 to 12 cm in length and from 4 to 6cm in width [Table - 1]. In all patients, donor sites were primarily closed. Operative technique Preoperatively using a handheld Doppler probe, adjacent Ulnar artery perforators were identified and marked. The potential reconstructive flaps were outlined in such a manner as to include the most distal and the best sounding perforator. The flaps were designed along the long axis of the vessels. Length of the flap taken was measured so that the distance between the perforator and the distal limit of the defect was equal to the distance between the perforator and proximal limit of the flap. The width of the flap was equal to the width of the defect and the flap was centered on the perforator. The final defect was created after devitalized tissue was debrided and the wound thoroughly irrigated. An exploratory incision was made along the radial margin of the proposed flap; sub fascial dissection was carried out to identify perforators supplying the flap. Perforators from the Ulnar artery were consistently observed in the distal half of the forearm. Once the perforators to the flap were identified the skin incision was then completed. Designing the flaps as an island with skeletonization of the distal perforators of the Ulnar artery facilitates the arc of rotation and avoids kinking of the pedicle. The flap was then islanded on a suitable perforator, and the remaining were temporarily micro clamped. The tourniquet was then released and perfusion of the flap confirmed. When a single chosen perforator supported the vascularity of the entire flap the other micro clamped perforators could be ligated safely. When a single perforator was not adequate, a second perforator was preserved. The selected perforator was freed from the fascia and dissected up to the Ulnar artery to acquire extra length, which would facilitate rotation of the flap. The flap was turned over distally over 180° to cover the defect and its margin was sutured to the edge of the defect [Figure - 2]. A drain was placed beneath the flap and the donor area was closed primarily. The hand was elevated to minimize postoperative venous congestion. Results The flaps survived in all patients. Although marginal loss over the distal edge of the flap was noted in one patient (Patient 6). This was managed with flap advancement and suturing. Mild edema developed in all patients and subsided over a time of two weeks except in one (Patient 5) where edema was moderate and subsided in about three months. In two patients where tendons were dead and were debrided, secondary reconstruction with tendon grafting was done, all other patients had normal gliding motion of involved tendons and joints and the cosmetic result in the donor site was good. A long term follow-up (mean, nine months) showed good flap durability and elasticity. Excellent results of two cases are shown. Patient 1 [Figure - 3]A, B, C, D, E and Patient 2 [Figure - 4]A, B, C, D. Discussion Soft tissue reconstruction of the volar aspect of the forearm and wrist for exposed vital structures remains a challenge for plastic and reconstructive surgeons. Skin defects may be covered by local, distant, or free flaps, depending on the conditions of the local wound, adjacent area, donor site and general condition of the patient. For reconstruction, early use of a flap with single-stage procedure that can provide well-vascularized flap coverage at the earliest, offers the best possible functional results with early rehabilitation, decreasing morbidity and hospital stay. Free flaps offer flexibility in size, shape, and positioning but are limited with regard to donor site morbidity and the need for a facility of microsurgery. Distant flaps including groin, inferior hypogastric and abdominal flaps provide enough tissue for reconstruction but require multiple-stage operations involving prolonged immobilization, increased morbidity and hospital stay. They are also bulky with sub optimal color match. Although local flaps are usually limited in size and mobility by the size and location of the defect, however if feasible, they offer relatively simple and safe wound coverage, spare the distant donor site for further reconstruction, and do not interfere with the patient′s activities and physical therapy. The de epithelialized turnover flap [1],[2] represents a reliable method, but there is donor site morbidity in terms of aesthetics and a large amount of skin graft is needed to resurface the wound. The local adipofascial turnover flap [3],[4] represents a reliable and simple technique for reconstruction if the surrounding soft tissue is available, but this is not always possible because of the limitation in terms of size and degree to which the flap can be raised. Random pattern fasciosubcutaneous flaps are based on the attached pedicle. As described in some reports [1],[5] the length-to base ratio is below 1.5:1, length-to-width ratio below 2.0:1, and flap-to-base area ratio below 4.0:1 are essential for flap survival. A useful flap for defects around the wrist is the flap described by Becker and Gilbert which relies on the dorsal branch of the Ulnar artery. The advantages of this flap are that it is a safe, simple and effective one-stage procedure providing thin, pliable, good quality skin with a robust blood supply. [6] Disadvantages of this flap are its short pedicle and its relatively limited arc of rotation and donor site morbidity. [7] Small size donor defects can be primarily closed otherwise they require split thickness skin graft. The posterior interosseous artery distally-based flap is suitable for the coverage of dorsal skin defects of the hand but can also be used for the volar aspect of the distal forearm and wrist and avoids interference with the two main arteries of the forearm. The dissection of the vascular pedicle, however, is frequently quite complex and tedious. It is necessary to have local healthy tissue around the wrist joint. If the distal perforators of the posterior interosseous artery and its branches are injured, the flap should be abandoned. [8],[9] Compared with other forearm flaps, our flap has a number of advantages. Distally-based island Ulnar artery perforator flap is a local flap, quick, easy to manage and aesthetically good. It is based on one or occasionally on two perforators. The flap is distally based which imports undamaged tissue into the primary defect and allows secondary defect closure easily. Islanding the flap facilitates the arc of rotation and avoids the pedicle kink when the flaps are turned 180 o and allows more distal reach of the flap, it therefore allows easier inset and has a better contour. Conclusion The distally-based islanded Ulnar artery perforator flap is versatile, safe and reliable for reconstructing defects of cosmetically sensitive areas like the wrist involving vital structure exposure. It provides aesthetically superior results, facilitates functional restoration and provides single-stage reconstruction without sacrificing the major artery of the forearm. The flap is suitable for closure of small or medium-size defects without donor site morbidity.References
Copyright 2007 - Indian Journal of Plastic Surgery The following images related to this document are available:Photo images[pl07006f3c.jpg] [pl07006f3d.jpg] [pl07006f4a.jpg] [pl07006f1.jpg] [pl07006f4b.jpg] [pl07006f2.jpg] [pl07006f3e.jpg] [pl07006f4c.jpg] [pl07006t1.jpg] [pl07006f3a.jpg] [pl07006f4d.jpg] [pl07006f3b.jpg] |
| |||||||||

![[Figure - 1]](/showimage?pl/photo/pl07006f1.jpg){kind=link}
![[Table - 1]](/showimage?pl/photo/pl07006t1.jpg){kind=link}
![[Figure - 2]](/showimage?pl/photo/pl07006f2.jpg){kind=link}
![[Figure - 3]A](/showimage?pl/photo/pl07006f3a.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![[Figure - 4]A](/showimage?pl/photo/pl07006f4a.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}