 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Plastic Surgery, Vol. 40, No. 1, January-June, 2007, pp. 18-24 Original Article Rigid internal fixation of zygoma fractures: A comparison of two-point and three-point fixation Atul Parashar, Ramesh K. Sharma, Surinder Makkar Department of Plastic Surgery, Postgraduate Institute of Medical Education and Research, Chandigarh - 160 012 Code Number: pl07007 Abstract Background: Displaced fractures of the zygomatic bone can result in significant functional and aesthetic sequelae. Therefore the treatment must achieve adequate and stable reduction at fracture sites so as to restore the complex multidimensional relationship of the zygoma to the surrounding craniofacial skeleton. Many experimental biophysical studies have compared stability of zygoma after one, two and three-point fixation with mini plates. We conducted a prospective clinical study comparing functional and aesthetic results of two-point and three-point fixation with mini plates in patients with fractures of zygoma.Materials and Methods: Twenty-two patients with isolated zygomatic fractures over a period of one year were randomly assigned into two-point and three-point fixation groups. Results of fixation were analyzed after completion of three months. This included clinical, radiological and photographic evaluation. Results: The three-point fixation group maintained better stability at fracture sites resulting in decreased incidence of dystopia and enophthalmos. This group also had better malar projection and malar height as measured radiologically, when compared with the two-point fixation group. Conclusion: We recommend three-point rigid fixation of fractured zygoma after accurate reduction so as to maintain adequate stabilization against masticatory forces during fracture healing phase. Keywords: Enophthalmos, fracture zygoma, malar height, malar projection, rigid internal fixation, vertical dystopia The zygomatic bone is the principal buttress between the cranium and the maxilla. Its convex shape and protrusion makes it more vulnerable to fractures in facial trauma. Displaced zygomatic fractures can result in significant malar flattening, ocular dystopia and enophthalmos. [1] Thus, treatment of these fractures must achieve adequate and stable reduction at the fracture site. A number of clinical and experimental studies have found strong evidence of superiority and better long-term fracture stability with the use of rigid plating system when compared with wire fixation in the treatment of zygomatic fractures. [2],[3] However, the precise stability of the zygoma with reference to the number of fixation points as well as the sites of rigid fixation still remain a topic of debate. [4],[5],[6] A few experimental biophysical studies have been conducted to compare the stability of fractured zygoma after one, two and three-point fixation with mini plates. There has been no clinical study which compares the results of two-point and three-point rigid plate fixation in patients with fractured zygoma. This study was conducted to address this particular aspect in the management of fractures of zygoma, so as to formulate an operative strategy that will achieve the surgical objective of stable fixation while minimizing the morbidity of the procedure. Materials and methods The study was conducted at Department of Plastic Surgery, Postgraduate Institute of Medical Education and Research, Chandigarh, a tertiary referral hospital between 1 st January 2002 and 30 th July, 2003. Patients with isolated zygomatic fractures reporting to the Plastic surgery emergency OPD between 1 st January 2002 and 31 st December, 2002 were included in the study provided they satisfied the following exclusion and inclusion criteria: Inclusion criteria
Informed consent was taken from all the patients before inclusion in the study. The study was also approved by Hospital Ethical Committee as it involved Open Reduction and Internal Fixation in accordance with standard treatment protocol being followed for fracture zygoma patients. Clinical assessment included detailed history and physical examination of the patients. Visual acuity, extra-ocular movements and presence of diplopia were recorded. Stratification of patients was done using simple random sampling into following categories: Group I: Patients to be treated with two-point fixation protocol (Fixation at fronto-zygomatic suture and inferior orbital rim) [Figure - 1]a. Group II: Patients to be treated with three-point fixation protocol (Fixation at fronto-zygomatic suture, inferior orbital rim and zygomatico-maxillary buttress) [Figure - 1]b. Computed tomography (CT) (axial and coronal) of midface was done to assess degree of displacement of the zygomatic bone. Numerical scoring of fracture zygoma (Cooter and David) [7] was done to document overall bony disruption among the two groups. Operative management of these patients included open reduction and internal fixation with non compression titanium mini plates. All patients were operated under general anaesthesia. Exposure of the zygomatic bone was achieved with lateral brow incision, subciliary incision and upper gingivo buccal sulcus incision. The extent of exposure was the same irrespective of the number of fixation points. After ensuring reduction and satisfactory alignment at all three fracture sites, mini plates were applied at two points (fronto-zygomatic suture and inferior orbital rim) in Group I patients and at three points (fronto-zygomatic suture, inferior orbital rim and zygomatico-maxillary buttress) in Group II patients. Wounds were closed in two layers after thorough irrigation. Patients were kept on weekly follow-up for the first two weeks and on monthly follow-up thereafter. After completion of three months patients were reassessed so as to record following parameters: Clinical functional assessment
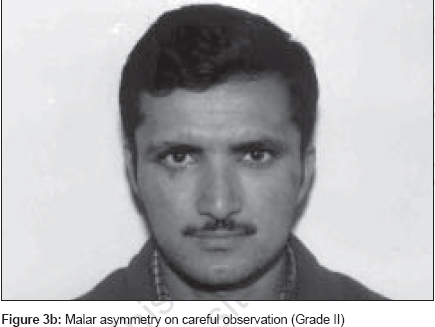
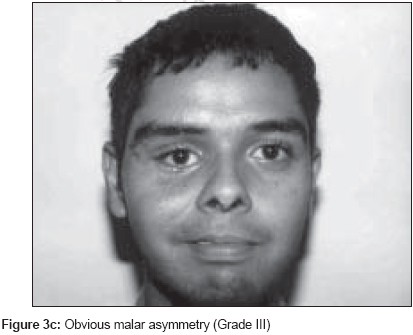
Aesthetic (photographic) assessment Frontal and basal views of the patients at three-monthly follow-up visits were assessed for malar depression and globe abnormalities by an experienced independent clinical investigator who was blinded to the type of fixation method used and results of other clinical parameters assessed. Grading of malar asymmetry was done according to the classification system proposed by Holmes and Mathews. [8] Each patient was assigned to one of the following grades [Figure - 3a], b and c. Grade I :
Excellent
cosmetic
result,
no
malar
asymmetry Globe abnormalities (dystopia and enophthalmos) were also recorded by the same investigator. Radiological assessment Post reduction displacement of zygoma was assessed radiologically for all the patients. CT scan of the midface was performed after three months of surgical rigid fixation. Zygomatic complex projection and zygomatic complex height (Furst et al ) [9] were measured as follows:
Results A total of 22 patients were included in the study. Twenty-one were males and one female with mean age of 28.45 years. The mode of injury was road traffic accident in 21 patients and fall from height in one patient. The average time lag between trauma and presentation was 1.18 days. The most common inspection finding was periorbital oedema (90.9%). Infra orbital sensations were diminished in 12 (68.18%) patients. The distribution of various signs and symptoms is shown in [Figure - 6]. The numerical zygomatic score varied from 3 to 5 with mean of 4.63. Twelve patients were treated with two-point fixation protocol and 10 patients were treated with three-point fixation protocol. Three patients developed infection at plating site. One patient belonged to Group II and two patients belonged to Group I. Location was zygomatico-frontal suture in all the patients and they responded to conservative treatment without the need for miniplate removal. Eighteen (81.81%) patients completed the three-month follow-up. Group I patients Clinical functional assessment: Ten (out of the initial twelve) patients reported for assessment at completion of three months. Vertical dystopia in this group ranged from 1mm to 3.5 mm with mean of 2.05 mm (SD 0.89). Enophthalmos ranged from 1 mm to 4 mm with mean of 2.4 mm (SD 0.96). Aesthetic (photographic) evaluation: Seven patients (70%) had Grade II malar asymmetry and three (30%) had Grade III malar asymmetry. Seven patients had enophthalmos and five patients had dystopia appreciable on photographic evaluation. Radiographic evaluation: Both malar projection and malar height were measured. The deficit in malar projection ranged from 2 mm to 6 mm with mean of 3.5 mm (SD1.35). The deficit in malar height ranged from 1.6 mm to 6.8 mm with mean of 3.74 mm (SD 1.76). Group II patients Clinical functional assessment: Eight patients (out of initial ten) reported for assessment at completion of three months. Vertical dystopia in this group ranged from 0 mm to 2 mm with mean of 0.81 mm (SD 0.75). Enophthalmos ranged from 0 mm to 3 mm with mean of 1.12 mm (SD 0.99). Aesthetic (photographic) evaluation: Five patients (62.5%) had Grade II malar asymmetry and three (37.5%) had Grade I malar asymmetry. Three patients had enophthalmos and two patients had dystopia appreciable on photographic evaluation. Radiographic evaluation: Both malar projection and malar height were measured. The deficit in malar projection ranged from 0 mm to 3 mm with mean of 1 mm (SD1.06). The deficit in malar height ranged from 0 mm to 4 mm with mean of 1.68 mm (SD 1.33). Comparison and statistical analysis of Group I and Group II patients Sampling variables: The mean age of Group I patients was 29.5 years and of Group II patients was 27.7 years. The difference between the two groups was not statistically significant. Mean zygomatic score (David and Cooter) [7] in Group I patients was 4.166 and of Group II patients was 4.5. The difference between the two groups was not statistically significant. Clinical parameters: Dystopia: The mean vertical dystopia in Group I patients was 2.05 mm and in Group II patients was 0.81 mm. The difference between the two groups was highly statistically significant ( P < 0.01). Enophthalmos : The mean enophthalmos in Group I patients was 2.4 mm and in Group II patients was 1 mm. The difference between the two groups was statistically significant ( P < 0.02). The findings are depicted in [Figure - 7]. Aesthetic (photographic) evaluation: In Group I seven patients (70%) had Grade II malar asymmetry and three (30%) had Grade III malar asymmetry. Among Group II patients five patients (62.5%) had Grade II malar asymmetry and three (37.5%) had Grade I malar asymmetry. The difference in the malar asymmetry profile of the two groups was not statistically significant ( P >0.1). Seven patients (70%) in Group I and four patients (50%) in Group II had photographically obvious globe position abnormalities in the form of dystopia or enophthalmos. However, this finding was not statistically significant owing to small sample size (Fisher Exact Test, P >0.1). Radiological evaluation: The mean deficit in malar projection in Group I patients was 3.5 mm (S.D. 1.35) and in Group II patients was 1 mm (S.D. 1.06). The difference was highly statistically significant (t=4.26, P < 0.001). The mean deficit in malar height in Group I patients was 3.74 mm (S.D. 1.76), while this parameter in Group II patients was 1.68 mm (S.D. 1.33). The difference between the two groups was statistically significant (t=2.73, P < 0.02). The findings are depicted in [Figure - 8]. Discussion The zygomatic bone has pyramidal shape with frontal, maxillary, temporal and orbital processes articulating with corresponding bones. Displaced zygoma fractures are vulnerable to secondary malposition as a result of masticatory forces even after some kind of fixation. [10] These forces must be overcome at fracture sites for optimal stabilization. [11] Any post-reduction displacement of zygoma can result in delayed development of malar asymmetry, dystopia and enophthalmos. Therefore the goal of treatment of zygomatic fractures is to restore and maintain pre-injury facial skeletal configuration. The biomechanics of the facial skeleton were investigated and discussed by Rudderman and Mullen. [12] According to them, fractured zygomatic segment has six possible directions of motion: translation across x, y and z axis; rotation about x, y and z axis. A miniplate applied across the fronto-zygomatic suture will resist translatory movement and also rotation along an axis perpendicular to the plane of miniplate because of the width of the plate. At the same time, it will offer little resistance to rotation along the linear axis of the plate. To improve stabilization, an additional plate is to be applied in a manner where the weak axis of both plates does not coincide with a line connecting them. A still more favorable situation can be created by choosing three fixation points that are not collinear. According to Pearl, [13] it is essential to reposition the zygoma at a minimum of three locations to achieve correction in three dimensions. He further opined that reduction at the fronto-zygomatic suture and inferior orbital rim can still leave persistent lateral rotation in the region of the anterior maxillary buttress leading to intra-orbital volume expansion behind the axis of globe. Many experimental biophysical studies have been conducted to find out post-reduction rotational stability of zygoma fracture after miniplate fixation. Davidson et al [1] analyzed different combinations of miniplate fixation for stabilizing fractured zygoma in human skulls. This experimental study found that three-point fixation at fronto-zygomatic suture; inferior orbital rim and zygomatico-maxillary buttress conferred maximum stability against forces matching physiological stresses. Similar results were found by O′Hara et al [14] in another experimental biophysical study. Despite these experimental studies, there were no prospective clinical studies analyzing the results of different fixation points. We have analyzed two commonly used fixation methods in an attempt to define the most appropriate method. Both the groups in our study were comparable in terms of age and extent of injury. Analysis of clinical parameters (dystopia and enophthalmos) revealed statistically significant variation among the two groups with the three-point fixation group (Group II) showing lesser postoperative displacement. Similarly, the deficit in the malar projection and malar height was more in the two-point fixation group. This finding was also statistically significant. The findings of photographic assessment also reveal better malar symmetry and less globe position abnormalities in the three-point fixation group. However, the difference in the two groups was not statistically significant. This could be due to the subjective nature of assessment as well as secondary to incomplete projection of actual bony deficits because of thickness of skin and subcutaneous tissue. Despite these apparent advantages, three-point fixation is associated with more extensive periosteal stripping, extreme retraction of bone edges and requirement of expert assistance for application of miniplate across the zygomatico-maxillary buttress. In addition, longer operative time, presence of more hardware and increase in cost of surgery are some disadvantages of fixation across an additional point. However, there were no additional complications (intra-oral suture line dehiscence, plate exposure) noticed in Group II patients. The analysis of these findings suggests that three-point fixation using mini plates provides better post reduction stability of zygomatic fractures against normal physiological tractive forces. It is associated with lesser incidence of vertical dystopia and enophthalmos while providing better malar projection and height. Conclusion Assessment of objective post fixation variables, viz. vertical dystopia, enophthalmos, malar projection and malar height show statistically significant enhancement in outcome attesting to better inherent stability of three-point fixation. Subjective assessment of aesthetic sequelae shows better results with three-point fixation though they do not achieve statistical significance in the present study, this could be because of the sample size of this study. We recommend three-point fixation with mini plates for management of displaced zygomatic fractures.References
Copyright 2007 - Indian Journal of Plastic Surgery The following images related to this document are available:Photo images[pl07007f2.jpg] [pl07007f4.jpg] [pl07007f7.jpg] [pl07007f1b.jpg] [pl07007f6.jpg] [pl07007f3c.jpg] [pl07007f1a.jpg] [pl07007f3a.jpg] [pl07007f3b.jpg] [pl07007f5.jpg] [pl07007f8.jpg] |
| |||||||||

![[Figure - 1]](/showimage?pl/photo/pl07007f1a.jpg){kind=link}
![[Figure - 1]](/showimage?pl/photo/pl07007f1b.jpg){kind=link}
![[Figure - 2]](/showimage?pl/photo/pl07007f2.jpg){kind=link}
![[Figure - 3a]](/showimage?pl/photo/pl07007f3a.jpg){kind=link}
{kind=link}
{kind=link}
![[Figure - 4]](/showimage?pl/photo/pl07007f4.jpg){kind=link}
![[Figure - 5]](/showimage?pl/photo/pl07007f5.jpg){kind=link}
![[Figure - 6]](/showimage?pl/photo/pl07007f6.jpg){kind=link}
![[Figure - 7]](/showimage?pl/photo/pl07007f7.jpg){kind=link}
![[Figure - 8]](/showimage?pl/photo/pl07007f8.jpg){kind=link}