 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
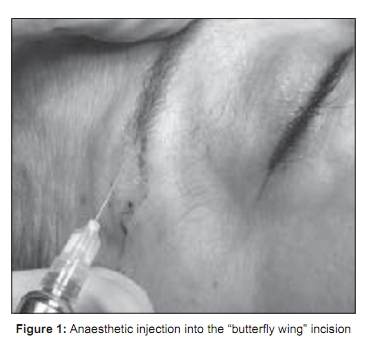
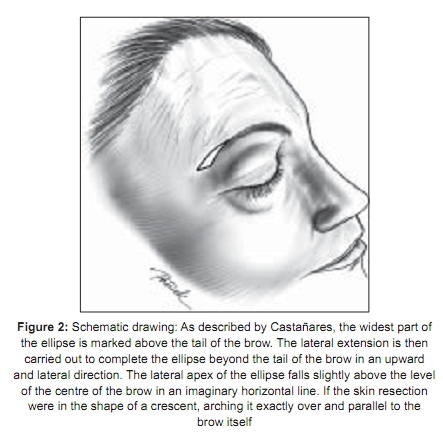
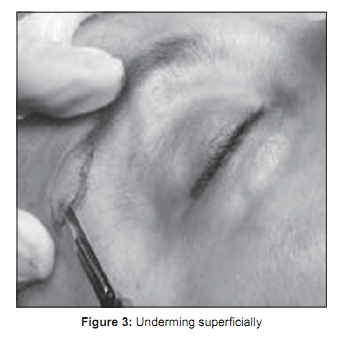
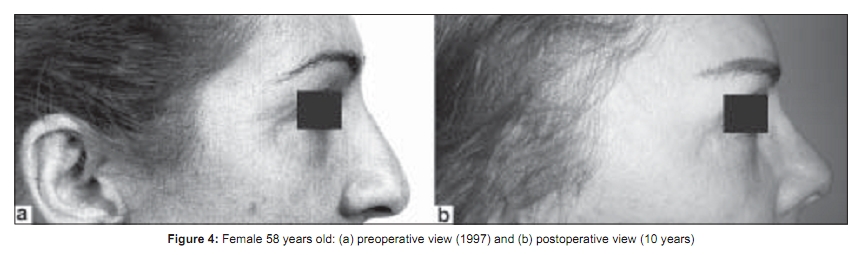
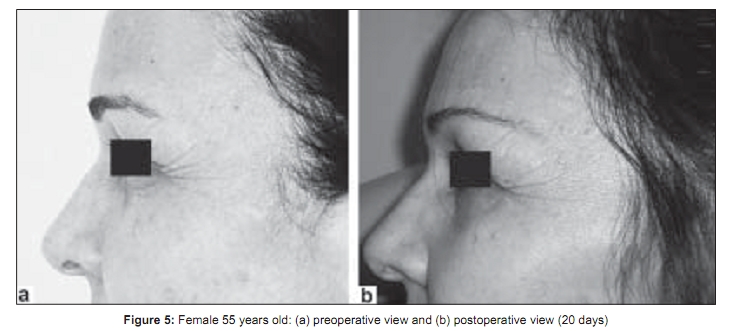
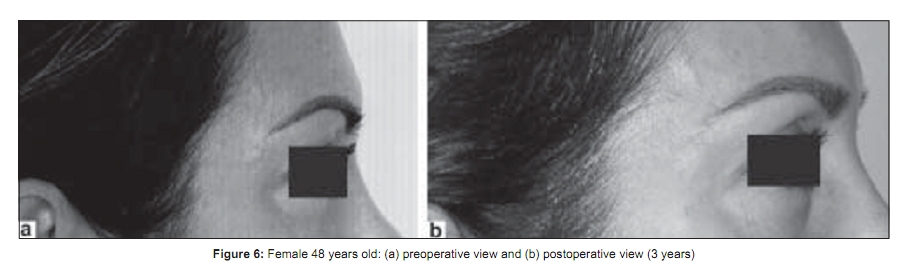
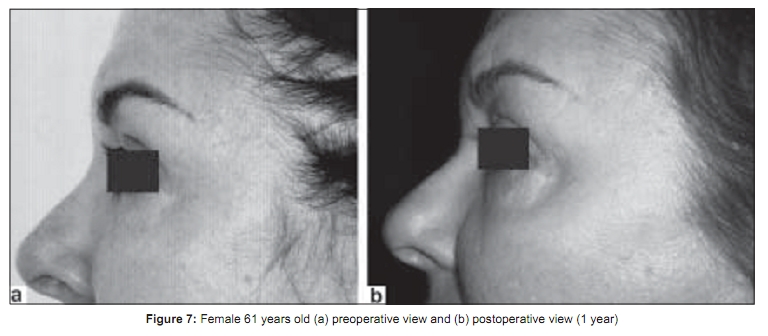
Indian Journal of Plastic Surgery, Vol. 42, No. 1, January-June, 2009, pp. 58-62 Original Article Approach to eyebrow ptosis through the modified technique of Castanãres Pires Viana Giovanni, Pires Viana Giovanni André1 Member of Brazilian Plastic Surgery Society, Member of Brazilian College of Surgeons, 1 Member of International College of Surgeons Correspondence Address: Dr. Pires Viana Giovanni André, Al. Jauaperi 732, São Paulo/SP, Brazil - 04523-013. info@cliniplast.com Code Number: pl09013 DOI: 10.4103/0970-0358.53013 Abstract One of the first signs of facial ageing appears in the forehead, with the descent of the lateral part of the brow. This is a troubling condition for all patients and elevation of the lateral part of the brow becomes a more and more frequent demand. The authors present their experience in 350 consecutive cases of direct eyebrow lift ("butterfly wing" incision) alone or in combination with rhytidectomy and/or blepharoplasty. The majority of the patients were female (90%). The age ranged from 43 to 85 years. Eighty per cent of the cases were performed simultaneously with rhytidectomy and blepharoplasty, 16% were performed in association with blepharoplasty and eyebrow lift alone represented 4%. The most common complication was epidermal cyst (3.4%) and suture dehiscence (2%). The "butterfly wing" incision provides a useful alternative to correction of eyebrow ptosis. Indication for surgery is dependent more on the ageing signs than on the patient's chronological age. The final results are consistently very gratifying to the patient and to the plastic surgeon alike.Keywords: Arched eyebrow; Eyebrow position; Eyebrow ptosis; Surgery for eyebrow ptosis Introduction Fascination with beauty as well as with the orbits and their surrounding tissues dates back to early human civilization. The lid-eyebrow region forms the emotional and expressive centre of the human face.[1] A high eyebrow positioned above the orbital rim and small eyebrows with the eyebrow arch positioned in the middle were preferred for many decades. [1],[2] Ageing causes decreased skin elasticity, which allows soft tissue to descend with gravity. Ptotic eyebrows can be hereditary, appearing early in life. The resultant brow ptosis manifests in lateral hooding of the eyelid and has implications for functional visual field obstruction as well as periocular cosmetic surgery. Surgical elevation of the forehead and brow for aesthetic improvement of the upper third of the ageing face has been performed for nearly 100 years. [3] Current methods of eyebrow lifting include direct eyebrow lifts, midforehead lifts, coronal brow lifts and endoscopic brow lifts. [1],[3],[4],[5],[6],[7],[8],[9],[10],[11],[12],[13] More recently, nonendoscopic, limited-incision approaches to correct the descent of the lateral eyebrow alone have been reported by several authors. [4],[6],[10],[14],[15],[16] The aim of this paper is to analyze the treatment of ptosis of the tail of the eyebrow by the modified technique of Castanãres in 350 consecutive patients who underwent direct eyebrow lift alone or in combination with rhytidectomy and/or blepharoplasty at a private clinic between January 1996 and December 2007. Material and Methods Between January 1996 and December 2007, 350 consecutive patients underwent a direct eyebrow lift alone or in combination with rhytidectomy and/or blepharoplasty. Each patient was evaluated for effective brow elevation, complications and overall satisfaction. Surgical procedure All patients were operated upon with monitored local anaesthesia. The local anaesthesic (2% lidocaine with 1:200,000 epinephrine) was injected into the "butterfly wing" incision [Figure - 1]. This drawing was proposed initially by Vinγs [5] and popularized by Castanãres. [4] The amount of skin resection depends on the elevation desired and the amount calculated ahead of time to be excessive. Viρas has suggested a simple but accurate method to determine the amount of skin resection: pinching the skin with the thumb and index finger above the lateral end of the brow with the patient in the erect position and watching for the desired effect. [5] After drawing the incision [Figure - 2] and injection of the local anaesthesic, the authors undermine superficially (epidermis dissection), like Schwartzman′s maneuver in breast reduction surgery [Figure - 3]. There is no undermining underneath this level. Then, the epidermis is removed and the closure is carried out in the conventional manner. A pressure dressing is applied to the incision for 5 days. Results 700 eyebrow elevations were performed in 350 consecutive patients whose ages ranged from 43 to 85 years. 90% of the patients were female. 90% of the cases were performed simultaneously with rhytidectomy and blepharoplasty, 16% were performed in association with blepharoplasty and eyebrow lift alone represented 4% of the cases. The procedure was completed on average in 30 min (20.45 min). The overall rate of complications was low. The most common complication was epidermal cyst (3.4%) and suture dehiscence due to local trauma (2%). Reoperation was performed in the unsatisfied patients (2%). There were no hypertrophic or keloid scars, no infection, no lagophthalmos and no post operative haematoma. The follow-up in this series was from 10 months to 11 years. Good brow elevation that lasted through the period of follow-up was uniformly demonstrated [Figure - 4],[Figure - 5],[Figure - 6],[Figure - 7]. Discussion The modern concept of "ideal" brow position was described by Westmore in 1974. [1],[15] However, there is a great diversity among individuals with respect to eyebrow position and shape and the notion of an "ideal" eyebrow has changed quite significantly over the past several decades, as demonstrated by Feser et al . [1] According to these authors there are atleast three ideals for a beautiful eyebrow; this being determined by the patients′ age for the young tend to prefer eyebrows in a lower position. This way, it seems plausible to assume that the trend currently appears to be moving away from arched eyebrows toward lower-positioned eyebrows with maximum height in the lateral third. [1] Knize discussed several mechanisms contributing to brow ptosis, including depression of the medial eyebrow from overaction of the brow depressors and descent of the lateral eyebrow from unopposed lateral orbicularis oculi contraction. [16] To recreate the aesthetically pleasing brow, several surgical procedures have been published over the past century. [3],[4],[5],[6],[7],[8],[10],[11],[12],[13],[14],[15],[16],[17] Many different surgical techniques and types of incisions for raising the brow have been characterized, including the classical approach correction through a transcoronal incision, [4],[5],[6],[7],[8],[13],[18],[19],[20] transpalpebral brow lift , endoscopic brow liftand the use of botulinum toxin.More recently, nonendoscopic, limited-incision approaches to correct the descent of the lateral eyebrow alone have been reported by several authors. [14],[15],[16] Sometimes a combination with brow lift and blepharoplasty is necessary to achieve the desired results.[13],[21] Performing upper blepharoplasty in conjunction with brow lift is not a problem if care is given to proper preoperative analysis, quantification and marking. [13] In this study, the authors present their experience with "butterfly wing" incision based on Viρas′ study. [5] Indication for surgery is more dependent on the ageing signs than on the patient′s chronological age. The author′s use this approach to correct the lateral end of the brow (tail), mostly in patients with hairless eyebrow or in patients wearing makeup to disguise the brow ptosis. Nevertheless, this approach would be carried out in all patients because they have been warned ahead of time of the scar extension. It is also important to stress to the patient that the scar would be visible for a period of time but it may be concealed temporrarily with cosmetics. Viρas [5] and Castaρares [4] correct the eyebrow ptosis by resection of a roughly elliptical section of the forehead skin immediately above and lateral to the eyebrow. Through this approach the forehead is undermined to the hairline, severing all epicranial fibres, the corrugator supercilii and the procerus. [4] The authors′ resection is performed superficially, like Schwartzman′s maneuver in breast reduction surgery, without undermining underneath the epidermis level. In this manner, the authors believe that this approach reduces the prevalence of unaesthetic scar formation by avoiding injury to the dermis. In this series, the most common complication was epidermal cyst (3.4%), suture dehiscence due to local trauma (2%) and reoperation of unsatisfied patients (2%). Reoperation was performed in seven patients with minimal recurrence of brow ptosis due to previous inadequate resection. Viρas et al . [5] revealed an extremely low complication rate (0.4%) of haematoma formation, permanent alopecia and "nerve damage". They also reported a 2.4% dissatisfaction rate, which is comparable with the numbers presented in this series and other studies in literature. [3],[5],[7],[8],[9],[13],[15],[16] According to Viρas, [5] the advantage of this approach is its simplicity, it is well tolerated as an outpatient procedure under local anaesthesia and that most patients can resume their activities the following day. The authors agree with Viρas in that the other advantage is that it carries a direct one-to-one correction of brow ptosis. The disadvantage of this procedure is the scars on the forehead. To quote Viρas: .The scars usually become inconspicuous with time. Also because of their location, they can be easily disguised (if necessary) with a couple of strokes of an eyebrow pencil". [5] If these factors are properly explained beforehand and with the visible improvement, these patients accept the temporary inconveniences with conformity and understanding. The "butterfly wing" incision provides a useful alternative in situations in which the surgeon may not be familiar with endoscopic techniques, does not have access to endoscopic equipment or when frontalis modification is not required. Although this operation yields sustained improvements, it does not remove all underlying factors involved in brow ageing. The effects of gravitational forces continue and may result in the need for future enhancements. The final results of this operation are consistently very gratifying to the patient and to the plastic surgeon alike. References
Copyright 2009 - Indian Journal of Plastic Surgery The following images related to this document are available:Photo images[pl09013f3.jpg] [pl09013f6.jpg] [pl09013f2.jpg] [pl09013f1.jpg] [pl09013f5.jpg] [pl09013f7.jpg] [pl09013f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}