 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
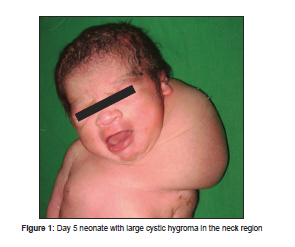
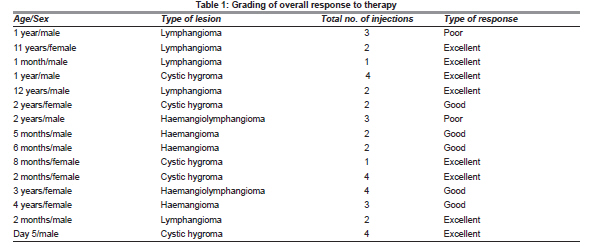
Indian Journal of Plastic Surgery, Vol. 44, No. 1, January-April, 2011, pp. 50-53 Original Article Bleomycin: A worthy alternative Gursev Sandlas, Paras Kothari, Parag Karkera, Abhaya Gupta Department of Pediatric Surgery, Lokmanya Tilak Muncipal Medical College and General Hospital, Sion, Mumbai, India Correspondence Address: DOI: 10.4103/0970-0358.81443 Abstract Context : Lymphangiomas are developmental anomalies presenting mainly in the first two years of life. Surgical excision has been the mainstay of treatment; however a potentially disfiguring surgery along with presence of important structures in the vicinity and infiltration into surrounding structures makes the dissection difficult.Aims : To study the safety and efficacy of Bleomycin as a sclerosing agent for lymphatic malformations in children. Settings and Design : Prospective non comparative nonrandomized trial. Materials and Methods: The study was carried out in 15 children between Day 5 of life to 12 years of age who presented between May2008 to May 2009. Bleomycin aqueous solution was injected intralesionally at a dose not exceeding 0.6 to 0.8 mg. /kg Body wt. The response to therapy was monitored clinically by measuring the length, breadth and area as well as by measuring the two largest perpendicular dimensions. The response was graded as excellent [total disappearance], good [>50% reduction] and poor [<50% decrease]. Those patients with diffuse lymphangiomas associated predominantly with hemangiomatous malformations, mediastinal, spinal or retroperitoneal extensions, visceral lymphangiomas, those with infections were excluded from the study. Statistical analysis used: None applicable. Results: The reduction in the size of the mass usually took between two weeks to ten months. The average duration of follow up has been ten months. A significant response was seen in 8 out of the fifteen [53.33%] patients. 5 patients [33.33%] patients showed a good response to therapy and achieved >50% reduction in the size of their swellings. 2 patients [13.33%] showed a poor response to therapy and achieved less than 50% reduction in the size of the swelling. Complications of the therapy were few and far between. 2 patients developed fever after injection, one patients reported a transient increase in size of swelling, 2 patients have developed discoloration of the overlying skin and are currently being followed up for final outcome. None of the patients developed leucopenia or leukocytosis. All of the complications were managed with conservatively. Patients are on long term follow up to evaluate long term effects, if any. Keywords: Bleomycin; sclerotherapy; lympangimatous malformations Introduction Lymphatic malformations are developmental anomalies presenting mainly in the first 2 years of life. [1] They have been classified into three major groups, although different varieties coexist. The cysts can vary from a few millimeters to several centimeters in diameter. [2] Surgical excision has been the mainstay of treatment; however, problems remain because of a potentially disfiguring nature of surgery, the presence of important anatomical structures in the vicinity which need to be protected and infiltration of the lesion into these structures making the dissection difficult. [1],[3] Coupled with a high-recurrence rate, there is a search for effective and safe alternative or adjuvant methods of treatment. This study was conducted to examine the efficacy of bleomycin aqueous solution as a sclerosing agent. And, although other alternatives are available, the concerned agent was used to evaluate its safety and efficacy in children. The study was conducted to evaluate the efficacy of intralesional bleomycin in cystic hygroma, lymphangiomas and haemangioma. It was a prospective study conducted at a tertiary care paediatric surgical centre in Mumbai. Materials and Methods The study was carried out in 15 children between Day 5 of life to 12 years of age who presented between May 2008 and May 2009. Those patients with diffuse lymphatic malformations with associated predominant haemangiomatous components, mediastinal, spinal or retroperitoneal extensions, visceral lymphatic malformations and those with infections were excluded from the study. An informed consent was obtained from the parents of the children subjected to intralesional bleomycin therapy in the out-patient department. After preliminary clinical examination and blood investigations, an imaging study that included ultrasound and magnetic resonance imaging in some cases was carried out where the extent was not clearly defined. Under complete aseptic precautions and necessary sedation, the lesions were aspirated as much as possible. The aspirating needle was kept in situ and bleomycin aqueous solution was injected intralesionally at a dose not exceeding 0.6-0.8 mg/kg body weight. [1] The multilocular lesions were aspirated and injected at multiple sites. The bleomycin was reconstituted in such a way as to deliver a dose of 0.5 mg/ml. The injection was repeated at an interval of 4 weeks and the cumulative dose of bleomycin was restricted to less than 5 mg/kg. The response to therapy was monitored clinically by measuring the length, breadth and area as well as by measuring the two largest perpendicular dimensions. Imaging for follow-up was restricted to cases that needed accurate assessment. The response was graded as excellent (total disappearance), good (>50% reduction) and poor (<50% decrease). The average follow-up period till now is 18 months, and patients are being followed-up regularly, and this is an ongoing process. Results Of the 15 patients treated, nine patients (60%) were less than 1 year of age. The youngest patient treated, a Day 5 neonate [Figure - 1], [Table - 1] had a huge lymphatic malformation in the neck. Nine patients were male and six patients were female. The most common site was the face and the neck region (10 patients); there was one patient with scalp haemangioma, one patient with inguinal region lymphatic malformation, one patient with suprascapular lymphatic malformation, one patient with a lip haemangioma and one patient with lymphatic malformation in the floor of the mouth. The reduction in the size of the mass usually took between 2 weeks to 10 months. The number of sittings varied from one to a maximum of four per patient. The average duration of follow-up has been 18 months. A significant response was seen in eight of the 15 (53.33%) patients. They showed an excellent response to therapy resulting in complete disappearance of the lesion [Figure - 2]. Five patients (33.33%) showed a good response to therapy and achieved >50% reduction in the size of their swellings [Figure - 3] and [Figure - 4]. Two patients (13.33%) showed a poor response to therapy and achieved less than 50% reduction in the size of the swelling. Both these patients had their swellings excised surgically. The patients showing a good response are currently under active follow-up. All of them have been given an option of surgical removal of the residual swelling, but they have opted for a wait and watch policy. The patients with excellent response have shown a good final cosmetic outcome with no signs of recurrence in any of them. Complications of the therapy were few and far between. Two patients developed fever after injection, one patient reported a transient increase in the size of the swelling and two patients had discolouration of the overlying skin and are currently being followed-up for final outcome [Figure - 5]. None of the patients developed leucopenia or leukocytosis. All the complications were managed conservatively and do not seem to have any lasting effects. Discussion Intralesional bleomycin as a sclerosing agent was used for the first time by Yura et al.[4] Bleomycin aqueous solution as a sclerosing agent has been used by many workers, and some of them found that it is not as effective as the bleomycin emulsion. Bleomycin has been shown to be more effective for cystic-type as compared with capillary or cavernous lymphangiomas. [1],[3],[5] Cervical, facial and axillary lymphatic malformations are more commonly composed of the cystic type. Pulmonary toxicity is a potential side-effect of bleomycin therapy. This risk is related to the dose, an increasing incidence being associated with a total dose of more than 400 units or a single dose exceeding 30 mg/m 2 of the body surface area. Elderly patients and those with underlying pulmonary disease are at an increased risk. [6] Because of the potential for airway compromise after bleomycin injection of some cervical lymphatic malformations, close monitoring is required for such lesions. [1],[3] We have not encountered any pulmonary complications in our study. The subjects are being screened with X-ray chest annually to look for early changes of pulmonary fibrosis. Intralesional bleomycin has been effective in complete resolution of the lesions in 60% of the patients, which is comparable, favourably, with the other studies carried out on this subject. [1],[2],[3],[5] A minimum dose of 1 mg/kg of bleomycin has been recommended in the literature for each injection of bleomycin. [1] However, we believe that this dose can be still lower and the sclerosing effect of the solution is still effective. In our study, we have used a maximum dose of 0.8 units/kg and have achieved comparable results. The desired effect of the drug locally is dependent on the availability of the drug per unit surface area of the lesion; [6],[7] hence, the amount of drug given should depend on the size of the lesion and not only on the weight of the patient. Another factor that can influence the final dose of the solution is the ability to aspirate the lesion before injecting. Uniloculate lymphatic malformations that could be successfully aspirated completely showed excellent response even at a lower dose and volume of the solution. However, the exact factors influencing the local action of the solution will need further detailed studies. References
Copyright 2011 - Indian Journal of Plastic Surgery The following images related to this document are available:Photo images[pl11010f4.jpg] [pl11010f2.jpg] [pl11010t1.jpg] [pl11010f1.jpg] [pl11010f5.jpg] [pl11010f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
![[Figure - 2]](/showimage?pl/photo/pl11010f2.jpg){kind=link}
![[Figure - 3]](/showimage?pl/photo/pl11010f3.jpg){kind=link}
![[Figure - 4]](/showimage?pl/photo/pl11010f4.jpg){kind=link}
![[Figure - 5]](/showimage?pl/photo/pl11010f5.jpg){kind=link}