 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Pediatric Neurology, Vol. 2, No. 3, July-Sept, 2004, pp. 166-170 CASE REPORT Temporary central hypoventilation following craniopharyngioma resection Sean M. Lew Sringarind Hospital, Khon Kaen University, Khon
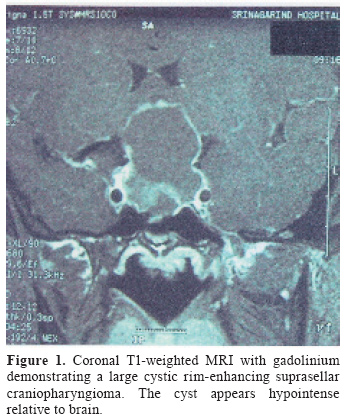
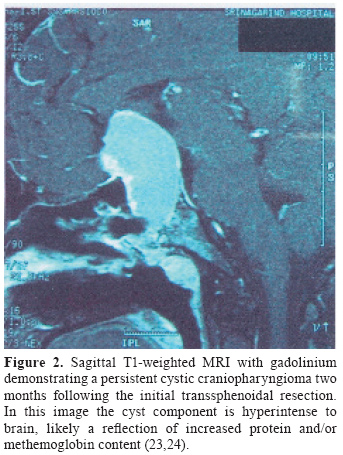
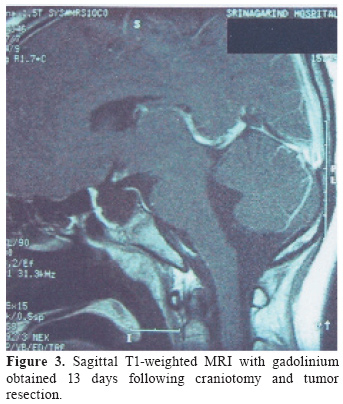
Kaen, Thailand Received: December 10, 2003. Revised: January 15, 2004. Accepted: January 21, 2004. Code Number: pn04033 ABSTRACT A case of temporary acquired central hypoventilation following craniopharyngioma surgery is presented. This is a complication which has not been previously described in suprasellar surgery. Potentially mechanisms of the respiratory disorder are discussed. The most likely etiology is felt to be respiratory drive depression stemming from hypothalamic injury. (J Pediatr Neurol 2004; 2(3): 166-170). Key words: hypoventilation, suprasellar surgery, craniopharyngioma, hypothalamus. INTRODUCTION Hypoventilation from neurologic causes (central hypoventilation) has been well described (1-4). While most cases are congenital in nature, numerous reports of acquired central hypoventilation exist. These reports almost universally involve patients with brainstem injury as the etiology of the hypoventilation (5-12). This is a case of temporary acquired hypoventilation following craniopharyngioma surgery, a complication not previously associated with surgery in the suprasellar region. CASE REPORT A 15-year-old girl presented to Sringarind Hospital (Khon Kaen, Thailand) with primary amenorrhea associated with a 3-year history of worsening vision. Her ophthalmologic examination revealed finger counting only OD, 20/200 OS, with bitemporal hemianopsia. Her neurologic examination was otherwise unremarkable. Secondary sex characteristics were normal. Preoperative laboratory values revealed an elevated prolactin level of 11.3 ng/ml and normal thyroid function tests. Magnetic resonance imaging (MRI) revealed a large cystic suprasellar mass felt to be most consistent with craniopharyngioma (Figure 1). A transsphenoidal resection was initially performed which resulted in obliteration of the cyst and improvement of vision. Surgical pathology was consistent with craniopharyngioma. She developed permanent diabetes insipidus postoperatively which was successfully managed with desmopressin. Postoperative computed tomography revealed residual solid tumor. Approximately two months postoperatively her vision worsened to 20/200 OU (before any adjunctive therapy had been initiated). MRI revealed recurrence of the cystic component of the tumor with persistent solid residua (Figure 2). She subsequently underwent a right orbito-pterional craniotomy. During this second procedure, all tumor was felt to have been removed with the exception of minute calcified flecks of capsule adherent to the underside of the right optic nerve. Hydrocortisone was administered in physiologic doses preoperatively and maintained intraoperatively and through the postoperative period. She remained sedated and intubated overnight. The following morning she was awake and following commands. Extubation was attempted later that evening but failed after one hour due to declining oxygen saturation and progressive hypercarbia. She was subsequently reintubated and her hypercarbia and hypoxia resolved rapidly with mechanically assisted ventilation. She maintained a normal level of consciousness. Over the ensuing 13 days she demonstrated marked hypoventilation and failed numerous attempts at weaning mechanical ventilation. Unassisted minute ventilation volumes remained low with low tidal volumes (ranging from 50-200 milliliters). During trials of pressure-support ventilation her respiratory rate would fall below normal during sleep. A clear cause of the hypoventilation was not identified. Her level of consciousness varied from mild somnolence to normal, but she was always easily aroused and communicated well. She remained afebrile after the second postoperative day. There was no evidence of meningismus. Nutritional status was adequate and maintained via nasogastric feeding. Electrolyte levels were within normal limits with the exception of mild hypernatremia that resolved by the second postoperative day. Endocrinological tests revealed normal thyroid functions and she remained on desmopressin and hydrocortisone maintenance. Liver function tests were within normal limits. Chest radiograms were unremarkable. MRI was obtained on the 13th postoperative day (Figure 3). This revealed a scant amount of enhancement in the hypothalamic/chiasmatic region. It was unclear if this represented elements of persistent tumor or early scarring given the time interval of the study after surgery (immediate postoperative imaging is not routinely obtained at this institution due to cost restrictions). Transcranial ultrasound was unavailable and the invasiveness of formal angiography was not felt to be warranted due to the low likelihood of significant vasospasm, particularly in the setting of her level of consciousness. Electroencephalography was not performed due to a lack of witnessed seizure activity and her otherwise normal mental status. She slowly demonstrated ventilatory improvement and was successfully extubated on the 14th postoperative day She was discharged to home two days later in good condition. Radiation therapy has not been performed and she will be followed by serial imaging for evidence of recurrence. DISCUSSION Neurologic causes of hypoventilation have been well described. Most cases of central hypoventilation are congenital, present in infancy, and are felt to be the result of primary defects of the brainstem respiratory centers (1-4). Acquired cases of central hypoventilation have also been reported, but predominantly in the setting of insults to the brain stem, including: hemorrhage (5), neoplasm (6-8), enlargement of the fourth ventricle (9), encephalitis (10), ischemia (11), and infarction (12). Interestingly, a small subset of spontaneous cases of central hypoventilation occur later in life and are associated with hypothalamic dysfunction, including hyperphagia, hypersomnolence, thermal dysregulation, and endocrinopathies (15,16). There is, in fact, ample evidence of a relationship between the hypothalamus and respiratory drive. In mammalian models, neurons of the paraventricular hypothalamus have been shown to project to respiratory centers in the medulla and spinal cord (17), and show changes in cellular activity that correlate with breathing patterns (18). Furthermore, in rats, neurons of the paraventricular hypothalamus modulate respiratory rhythm when activated directly via microinjection of neurotransmitters (19,20). Human studies have shown a relationship between leptin, a protein hormone produced in adipose tissues, which acts on receptors in the hypothalamus, and hypoventilation (21,22). Finally, functional neuroimaging has demonstrated activation and deactivation of the hypothalamus (as well as other centers of respiratory control) during respiratory challenges (23,24). A surgical insult to respiratory centers within the hypothalamus may have resulted in the transiently diminished respiratory drive seen in this patient. This hypothesis is based on the lack of other apparent causes of her state, the well-known association between craniopharyngioma surgery and hypothalamic injury, and the evidence of a relationship between the hypothalamus and respiratory drive in both animal models and human physiologic studies. It is possible that in most cases of hypothalamic surgical insult the mental status is more profoundly affected which makes a potential diagnosis of central hypoventilation more difficult to reach, as it is a diagnosis of exclusion. This is the first report of acquired central hypoventilation associated with surgery on a suprasellar tumor. REFERENCES
Copyright 2004 - the Society of Pediatric Science, Yüzüncü Yil University, Faculty of Medicine, Department of Pediatric Neurology, Van, Turkey The following images related to this document are available:Photo images[pn04033f3.jpg] [pn04033f1.jpg] [pn04033f2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}