 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Pediatric Neurology, Vol. 2, No. 4, Oct-Dec, 2004, pp. 225-229 CASE REPORT Macrophagic myofasciitis in a 3-month-old child * Mehar C. Sharma 1, Anibal Prentice 2, Peter F. Schmidt 3, Naresh Sharma 4, Hans H. Goebel 1 1 Department of Neuropathology, Johannes Gutenberg-University Mainz,
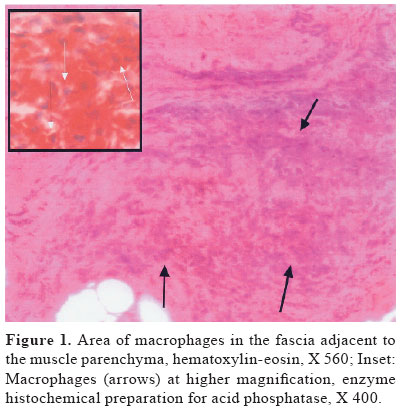
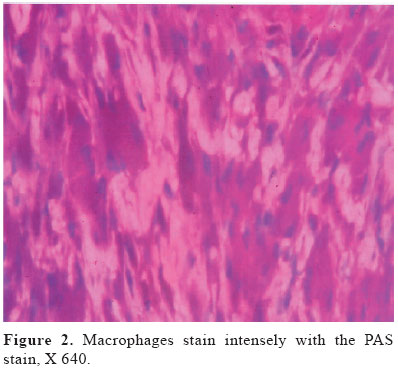
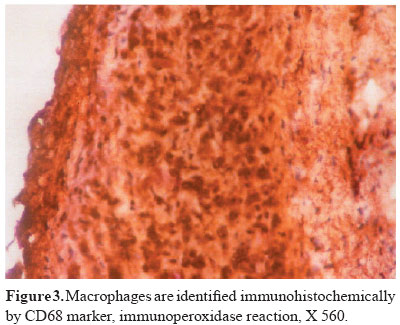
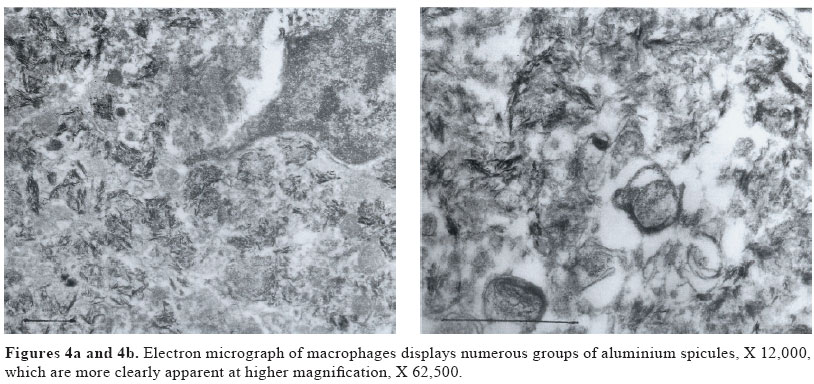
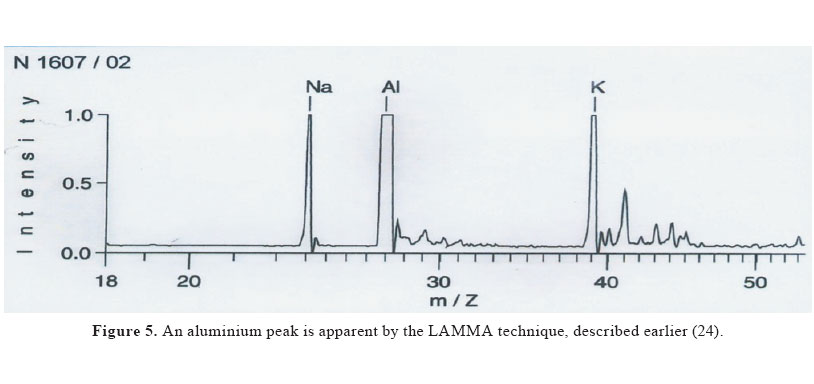
Germany Received: February 13, 2004. * This paper was presented at the Winter Meeting of the French Neuropathological Society, Paris, 2003. Code Number: pn04043 ABSTRACT Macrophagic myofasciitis (MMF) is a rare inflammatory myopathy which occurs after injection of aluminium-containing vaccines against hepatitis B virus (HBV), hepatitis A virus, and tetanus toxoid. Most of the cases reported are from France and are adult patients. We report a rare case of MMF in a 3-month-old male child of Indian origin. He was immunized for HBV at birth after which he developed generalized hypotonia, and central nervous system and peripheral nervous system manifestations at 1 month of age. Muscle biopsy showed typical features of MMF and aluminium could be detected in the muscle biopsy macrophages by ultrastructural examination and LAMMA technique. Our case is the youngest case of MMF and one of few from Asia. (J Pediatr Neurol 2004; 2(4): 225-229). Key words: macrophagic myofasciitis, inflammatory myopathy, vaccine, aluminium, child. INTRODUCTION Macrophagic myofasciitis (MMF) is a rather recently recognized entity, emerging from France (1) in 1993. This name MMF was coined by the French Study and Research Group on Acquired Dysimmunity-related Muscle Diseases (GERMMAD) for a putative inflammatory myopathy. To date, more than 130 cases have been reported, mostly from France (2) but a few also from other countries including USA, UK, Germany, Portugal, Spain, Italy (3-7) and, most recently, Israel (8). The majority of cases documented are adults with few exceptions (3,6-9). We report a rare case of MMF in a 3-month-old Indian child, who is the youngest reported case and one of few from Asia (8), to the best of our knowledge. CASE REPORT This boy was the second child in a consanguineous marriage. His antenatal period was uneventful. He was born by normal vaginal delivery without any complications and Apgar score at birth was 8 and 9. He weighed 3029 grams. He was given BCG and Engerix B injections vaccine against hepatitis B virus (HBV) and discharged on the fourth day. Both parents as well as his elder brother, who is 2 years old, are healthy without any muscle disease. On the 12th day he presented with respiratory stridor and weakness, but was discharged after one day in hospital. At 1 month of age he presented with generalized muscle hypotonia and respiratory failure requiring ventilatory support. His mother noted that he was sleeping all the time and did not feed well. He had decreased spontaneous movements and respiratory stridor. Tendon reflexes were brisk and occasional ankle clonus was present. Later on, he developed apneic spells and generalized seizures. Weaning off from respirator was transiently successful. Routine hematology, serum, biochemistry, and detailed work up for inherited metabolic disorders did not reveal any abnormalities. creatine kinase level was 112 U/L. C-reactive protein was 95 mg/dL (Normal: < 6 mg/dL). Electroencephalogram (EEG), done twice, revealed sharp waves in the right temporal and parietal regions and diffuse low voltage consistent with an encephalopathy, and epileptiform discharges were also seen. Electromyography showed few fibrillation potentials in biceps muscle and normal motor unit potentials (MUP). Further electromyographic examination with a concentric needle electrode was performed in the right tibialis anterior, rectus femoris, deltoid and abductor pollicis brevis muscles. Fibrillation potentials were found in all muscles examined with neurogenic repetitive discharges. Small MUP of brief duration were also seen. Nerve conduction velocities (NCV) of median and tibial nerves were 17.4 m/sec (normal for age 29 ± 2.5 m/sec) and 19 m/sec (normal for age 25 ± 2.0 m/sec), respectively, with small compound motor action potentials CMAPs. Magnetic resonance imaging of the brain did not reveal evidence of white matter disease. Muscle biopsy from the left thigh was performed to rule out any neuromuscular disorder. Myopathologic examination The muscle biopsy specimen was conventionally divided into two portions, frozen, and embedded in epoxy, and processed in the standard way. Frozen sections showed adipose tissue and transversely cut muscle fibres. There were sheets of cohesive, medium-sized macrophages with bluish cytoplasm and vesicular nuclei with prominent nucleoli which were predominant in the adipose and connective tissues (Figure 1) but, at places, infiltrating the endomysium centripetally. Muscle fibres showed mild variation in fibre size, regionally surrounded by endomysial fibrosis. No vasculitis was seen. These macrophages were positive with PAS stain (Figure 2) and for acid phosphatase activity (Figure 1, inset). Immunohistochemistry revealed strong expression of CD68 (Figure 3), MHC-I, MHC-II, LFAb, and ICAM-1 on macrophages but not on myofibres. A few T-lymphocytes were also identified amidst these macrophages. Perifascicular atrophy was not evident, and there was no deposition of MAC complex (C5b9). Well-formed granulomas and giant cells were not seen. Special stains revealed no organisms. Ultrastructural examination showed numerous irregular membrane-bound collections of fine, needle-shaped, randomly oriented inclusions in macrophages (Figures 4a and 4b). LAMMA technique revealed a single peak of aluminium in several areas of epon-embedded semithin sections (Figure 5), thus, further detailing light and electron microscopic findings. DISCUSSION MMF was first described from France by Gherardi et al. (1), as an unusual myopathy, probably of infectious etiology, but they could not find the nature of the infectious agent. However, histopathological features of all cases described, including the case under discussion, are stereotyped. Muscle biopsy tissue shows perimysial and peripheral endomysial infilteration by bluish, granular, PAS- and CD68-positive macrophages with occasional intermingled T lymphocytes. Myofibres show no or minimal myonecrosis. Absence of well-formed granulomas, necrosis, Langhans type of giant cells, and vascular changes exclude the possibilities of sarcoidosis, tuberculosis, and fasciitis-panniculitis syndromes like Shulman’s disease, toxic oil syndrome and eosinophilia-myalgia syndrome (10,11). An infectious etiology, as is Whipple disease, has been disproven based on response to antibiotics treatment (12-14) since no Tropheryma Whippelii could be denonstrated by staining as well as polymerase chain reaction (2). However intracytoplasmic osmiophilic spiculated structures in the macrophages, which resemble apatite crystals of unknown significance (1), are in fact aluminium hydroxide crystals (2). These crystals were also found in our case and their nature was further confirmed by LAMMA technique which showed a single peak of aluminium, as also observed by other authors (3). Authier et al. (15) reviewed 92 patients of MMF from France and found that all had a history of immunization with aluminium containing vaccines, i.e. HBV, hepatitia A virus, and tetanus toxoid (TT). The time interval between vaccination and muscle biopsy ranged from 3 to 78 months (median 33 months). This theory of causative relationship with aluminium is not new. Mrak et al. (16). in 1980, reported a case of centronuclear myopathy with unusual granulomatous inflammatory infiltrate in an autopsy case, which was attributed to previous biopsy. However he reproduced similar granulomatous lesions in rats vaccinated with DPT (diphtheria-pertussis-tetanus) vaccine (16). Similar granulomas have been described in subcutaneous tissue after vaccination with an aluminium-contaning adjuvant (17-20). The majority of reported MMF patients are adults and presented with generalized myalgia and chronic fatigue (1,2). However, these patients rarely present with central nervous sytem (CNS) manifestations like multiple sclerosis in the form of a demyelinating disease (15). MMF in children is rare and only eleven children have been reported (3,6-9). Because of rarity of MMF in childhood, symptomatology in children is not completely known unlike that in adult patients. Interestingly, few of the earlier reported children also presented with hypotonia (3,6,8) like our patient. Lacson et al. (3) reported two male children with MMF, aged 5 and 6 years, respectively, the latter patient presenting with developmental delay, poor head control and truncal hypotonia.The patient reported by Navarro et al. (6) was 16 months old and presented with congenital hypotonia. Di Muzio et al. (7) reported MMF in a 1-year-old child who presented with irritability, delayed motor development, and hyperCKaemia. Examination of the child showed mild hypotonia of the lower limbs. A recent cohort of six Muslim Arab children ranging in age between 4 and 40 months at the time of muscle biopsy, revealed a variety of central nervous system conditions and MMF as unrelated and, thus, coincidental findings. Muscle hypotonia in each patient had prompted muscle biopsy at a site of earlier vaccination. Aluminium was identified in macrophages, but inflammatory cells were often absent from the biopsied muscle tissue (8). Based on EEG findings and decreased NCV values, we presume that our patient developed a CNS disease and peripheral neuropathy. Authier et al. (15) reported that 14 of 92 patients (15%) in their series developed CNS manifestations, and 8 of them fulfilled the criteria for multiple sclerosis and were symptomatic (15). Our patient, however, did not show radiological evidence of CNS involvement. The reported interval between CNS manifestations and vaccination varied from 3 to 66 months. Therefore, it is possibile that MRI was done too early to pick up these changes. Based on our above findings the patient had an unquestionable axonal peripheral neuropathy of diffuse and moderate severity. Small MUP indicate myopathy but these changes can also be seen in early denervation and reinnervation. The significance of peripheral nervous sytem (PNS) involvement in the form of abnormal NCV values is not clear to us and has not been reported earlier. The local response at the site of injection is related to a chronic immune response in relation to aluminium-containing vaccines but MS-like manifestations are probably due to exaggerated response or altered immune response. Acute demyelination or MS-like manifestations had also been reported after HBV vaccination (21). Since these presentations are rare after vaccination, the alternate hypothesis is of genetic susceptiblity, i.e. some individuals are more susceptible to MMF than others. This theory is further corroborated by the fact that MMF has been reported in identical twins (22) and also in association with autoimmune diseases and inclusion body myositis (23). Although MMF is a rare complication of aluminium-containing vaccines, this possibility should be considered, not only in adults but also in children. After vaccination children should be closely followed to detect these complications at early stages. ACKNOWLEDGEMENT We thank Dr. R.K. Gherardi (Paris/France) for advice, Mr. W. Wagner for photography and Mrs. A. Wöber for editorial assistance. REFERENCES
Copyright 2004 - the Society of Pediatric Science, Yüzüncü Yil University, Faculty of Medicine, Department of Pediatric Neurology, Van, Turkey The following images related to this document are available:Photo images[pn04043f1.jpg] [pn04043f4a-b.jpg] [pn04043f3.jpg] [pn04043f5.jpg] [pn04043f2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}