 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Tropical Journal of Pharmaceutical Research, Vol. 1, No. 2, December, 2002 pp. 55-66 Identification of Standards for Pharmaceutical Care in Benin City Patrick O Erah† and James C Nwazuoke Pharmacotherapy Group, Faculty of Pharmacy, University of Benin, Benin City,
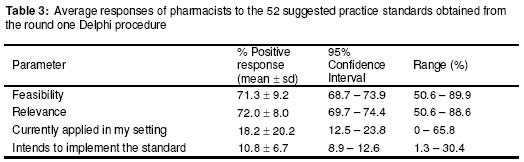
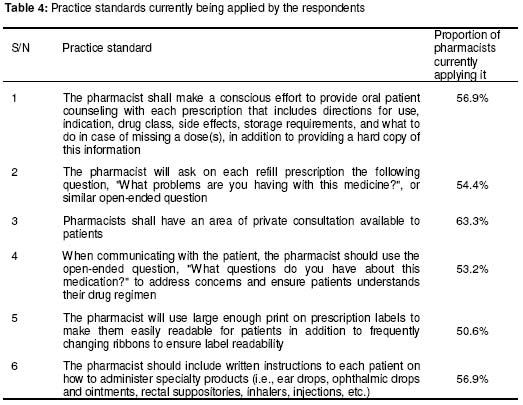
Nigeria Code Number: pr02009 ABSTRACT Purpose: Pharmaceutical care (PC) is still a theoretical statement in Nigeria and not operational. The goal of this study is to identify practice standards that can be effectively applied in the implementation of pharmaceutical care in Nigeria. Keywords: Benin City, pharmaceutical care, practice standards INTRODUCTION Pharmaceutical care is a process in which a pharmacist co-operates with a patient and other professionals in designing, implementing and monitoring a therapeutic plan that will produce specific therapeutic outcomes for the patient. These outcomes are: cure of a disease, elimination or reduction of a patient's symptoms, arresting or slowing a disease process or preventing a disease or symptoms1. Pharmaceutical care involves identifying, resolving and preventing drug-related problems. Since it was first defined by Hepler and Strand1 in 1990 as “the responsible provision of drug therapy for the purpose of achieving definite outcomes that improve a patient's quality of life, the care has taken on a wide variety of meanings to researchers and pharmacy practitioners and the operational definition range from the mandatory counseling to patient assessment and the development of patient care plans2. Many more definitions have now emerged and Cipolle and his colleagues have redefined it as “a practice in which the practitioner takes responsibility for a patient's drug-related needs and is held accountable for this commitment3. This latter definition has three components which are: (1) a philosophy of practice, (2) a patient care process, and (3) a practice management system. Most major pharmacy organizations in developed countries (e.g., the American Pharmaceutical Association [AphA]4 and the American Society of Health-System Pharmacists5) have since adopted the pharmaceutical care philosophy. Pharmaceutical care evolved from clinical pharmacy practice (which evidently emerged in Nigeria in the 1980's with the introduction of clinical pharmacy courses in the Faculty of Pharmacy, University of Benin, Benin City). The philosophy has achieved great successes in the care of patients in the United States and elsewhere. Patients now get better care from pharmacists, and the pharmacists, the patients and health care managers are delighted about the initiative. However, among the pharmacists in Nigeria, pharmaceutical care is often discussed in continuing professional education programmes and in conferences, and it is only yet considered as a model that needs to be implemented in the health care system. Admittedly, the standard of pharmacy practice in Nigeria is not the same as it is in most other countries. If nothing else, the practice settings are different. One of the interesting things about health care in Nigeria is that private patients entering the hospitals have to pay for their own food, bedding, bandages, medical supplies, drugs and other products essential to proper care and healing. In many cases, patients or their families have no money to pay for drugs and other necessities. Other factors that are potential barriers to pharmaceutical care are those already identified and include: (1) not enough time to talk with patients, (2) lack of private counseling area in the pharmacy, (3) inadequate training, (4) pharmacist's perception that patients are not willing to pay for this intensive level of care and (5) trepidation regarding the reaction of physicians6-10. These factors are not only compromising the early implementation of pharmaceutical care in hospitals and community pharmacies in Nigeria but have also had negative consequences on the impact of clinical pharmacy practice in the health care system in the country. Despite these problems, pharmaceutical care poses great challenges before the pharmacy profession in Nigeria. The challenges need to be addressed in order to move the care from a theoretical statement in Nigeria (as it is now) to an operational level. If all pharmacists are expected to universally deliver pharmaceutical care, they should adopt practice standards that provide meaning to the term and enable a holistic view of patient care. The answer to a fundamental question on whether the standards should be consistent regardless of various practice settings is that although the goals of pharmaceutical care exist independent of practice setting, the specific content of standards may vary from setting to setting1. Also, lack of standards for pharmacists to conform to in daily practice has been identified as a primary obstruction to widespread implementation of pharmaceutical care2. Already, a Delphi panel of pharmaceutical care experts has suggested 52 practice standards2 upon which a consensus was arrived at in the United States. This opens a lead way for the identification of standards that can effectively be applied in pharmacy practice in Nigeria. The primary intent of this study was to identify standards that can be effectively applied in implementing pharmaceutical care practice in Nigeria. The specific objectives are (1) to identify pharmaceutical care practice standards that can be effectively applied in Benin City, and (2) assess which of the practice standards are feasible, relevant and currently being applied or intended to be applied in Benin City. With the introduction of the Doctor of Pharmacy programmes in the training of pharmacists in Nigeria (which has already taken-off in the University of Benin, Benin City), the outcome of this study should create new knowledge with both theoretical and practical implications. In addition to reporting opinions or judgements, the study will provide a basis for changes in pharmacy practice and a framework for the implementation of pharmaceutical care practice in Nigeria. METHOD This study was carried out in Benin City, a large metropolitan city located in the south-south geopolitical zone of Nigeria. The city has a projected population of about 1.2 million. There are three tertiary health care facilities; a 550-bed University of Benin Teaching Hospital (UBTH), a 400-bed Edo State Government controlled Specialist Hospital and a Psychiatric Hospital. Each of these facilities has pharmacy departments under the control of registered pharmacists. There is also a Military Hospital and at least 150 registered community pharmacies, providing pharmaceutical services to the population under the supervision of pharmacists. At the time of this study (January to June 2002), there were about 211 registered pharmacists in Benin City. There are several other health care facilities including private hospitals, doctor's clinics or surgeries, maternity homes and herbal homes where pharmaceutical services are not being provided by qualified pharmacists. In all the health care facilities, the pharmaceutical care practice is not currently being effectively applied and clinical pharmacy practice is only marginally evident in the tertiary health care facilities. Apart from one community pharmacy where clinical pharmacy practice is obvious, all the community pharmacies engage in traditional drug retailing and distribution. The survey instrument (pre-tested self-administered questionnaire) for this study was constructed based on the 52 suggested practice standards obtained from the round one discussion by the Delphi panel of pharmaceutical care experts (see Appendix)2. The questionnaire contained the initial 52 suggested practice standards with spaces provided for indicating age, gender, qualification, practice area and year of experience, and whether each standard was feasible or not feasible, relevant or not relevant, currently applied in his/her establishment or not currently applied, and there was plan to implement it in his/her establishment or not. One hundred and fifty (150) copies of the questionnaire were distributed to qualified pharmacists who were in academics, hospital practice or community practice. Academic pharmacists were included in this study because they are involved in the training of pharmacy undergraduates and continuing professional education of qualified pharmacists. They are also frequently involved in the development of guidelines and standards of practice in pharmacy. The questions were distributed to the pharmacists in their offices. The researchers discussed the purpose of the study with each of the participating pharmacists, and educated them on the questionnaire format and how to indicate the desired response in the appropriate space provided in the questionnaire in order to prevent errors in responses. The copies of the questionnaire were left with the pharmacists who voluntarily accepted to participate in the study and retrieved from them within a period of two weeks after one to three visits. Those who were unable to fill the questionnaire by the third visit were considered as non-respondents because of time considerations. Each questionnaire used in this study was coded for easy reference. The responses from the study were fed into computer software, Epi Info 2000 (CDC, USA/WHO, Geneva) and double-checked to ensure accurate data entry. The data were analysed in terms of demographic characteristics, professional experience, qualification and practice areas (academic, hospital or community practice) using frequencies and percentages as appropriate. In analyzing the responses on current application and intention to apply the practice standards, only responses from pharmacists working in hospitals and community pharmacies were considered. This approach was adopted to prevent bias as nearly all the pharmacists in academia were full-time University Lecturers not involved in patient care. Chi-square test was adopted in estimating possible differences in proportions. Analysis of variance was used to determine differences between the age of the pharmacists, years of professional experience, qualification, practice areas and the responses to the suggested practice standards. For this purpose, the frequencies of responses for each suggested standard were determined based on age, years of experience, qualification and practice areas. At a confidence interval of 95%, a 2-tailed probability (p) value less than or equal to 0.05 was considered to be significant. Statistical comparisons were made using a software called Instat (GraphPad Inc., USA). RESULT Of the 150 copies of the questionnaire distributed to the pharmacists, 119 completed and returned the questionnaire, giving a response rate of 79.3%. All PhD holders were in academic setting and responded to the questionnaire. The age and sex distribution of the responding pharmacists are given in Table 1. A statistical gender balance was not achieved in this study (p < 0.04). The highest proportion (30.3%) of the respondents were aged from 31 - 40 years while the lowest proportion were in the age range of 51 - 60 years. The distribution of the respondents in respect of their qualifications, area of practice and years of experience are presented in Table 2. Majority of the respondents (71.6%) hold only a first degree in pharmacy. The rest had further higher education (master's degree, fellowship and PhD). The highest proportion of the respondents practice in community pharmacies (47.8%) and had not more than five years experience as pharmacists. The positive responses to the 52 suggested practice standards are summarized in Table The positive responses to the 52 suggested practice standards are summarized in Table 3. With respect to feasibility, the average positive response was 71.3%. Each of the practice standards with positive responses below 60% is marked with asterisk (*) in the Appendix (The 52 suggested practice standards obtained from the round one Delphi procedure). The highest positive responses on feasibility were on the need for the pharmacist to (1) devise a standard system of data collection of all necessary medical and personal information from each patient (89.9%), (2) document follow-up care plan and where care plan is not deemed necessary (88.5%), and (3) formulate therapeutic plan for the patient (83.5%). On the question of the relevance of each of the practice standards, the average positive response (72.0%) was not significantly different from that of the responses for feasibility (p > 0.05). Not less than 50% of the pharmacists judged all the initial 52 suggested practice standards to be both feasible and relevant. However, not less than 60% of the pharmacists judged 47 of the suggested practice standards to be both feasible and relevant. The responses on current application of each of the standards (mean ± sd, 18.2% ± 20.2%; 95% confidence interval, 12.5% - 23.8%) were generally low when compared with those of “relevance” and “feasibility”. The suggested standards currently applied by over 50% of the respondents are given in Table 4. Also, the responses on the intention to apply the standards in the respondents’ practice area were relatively low (mean ± sd, 10.8% ± 6.7%; 95% confidence interval, 8.9% - 12.6%).. In this study, analysis of variance did not reveal any significant difference between the years of experience, qualification, or practice areas and the responses to the suggested practice standards (p > 0.05). DISCUSSION Drug therapy with prescribed medication is a collaborative process involving the patient, the physician, the pharmacist and other health care professionals. In recent years, pharmacists in many countries have adopted a much more patient centred approach in the pharmaceutical services they provide. This assures that both patient care and economic aspects of drug therapy are appropriately considered in the interest of the patient. The principles of pharmaceutical care are embedded in the concept of Good Pharmacy Practice11. Application of practice standards that are practicable can result in enhancement of clinical, economic and humanistic outcomes of patient care12-14. In arriving at practice standards that can be applied in Nigeria, this study has adopted this survey approach as a framework, using known standards that have been previously applied in arriving at practice standards elsewhere2. The need for pharmacists to agree on a standardized approach by which individual pharmacists will provide pharmaceutical care to patients cannot be overemphasized. There is no doubt that pharmaceutical care will fail if each pharmacy setting or individual pharmacists are allowed to define pharmaceutical care standards on their own15 . The involvement of pharmacists in any setting in developing practice standards for pharmaceutical care to which they can adhere and upon which they may ultimately be evaluated is relevant2. It is for these reasons that only qualified pharmacists were involved in this study. Designed to provide a framework for developing standards that will be acceptable to pharmacists in Nigeria, and in particular, Benin City, and which they can meaningfully apply, this study has considered a good spread in the age, years of experience, qualification and practice areas as well as gender balance in its conduct. Although a statistically significant gender balance was not achieved in the study sample it is unlikely that the result obtained would change significantly if a gender balance was achieved. Neither the age, years of experience, qualification and practice areas was found to have significantly affected the responses from the responding pharmacists. The possible reason for this finding is that the introduction of the term, “pharmaceutical care” in the practice of pharmacy in Nigeria is new. Furthermore, pharmacists in Benin City are still trying to apply the philosophy with the hope that they will achieve a better health care provision. On the issue of feasibility and relevance of the Delphi initial 52 practice standards, it is difficult to recommend all the standards for initial application in Benin City even though more than 50% of the responding pharmacists have indicated the feasibility and relevance of all the standards. The practice standard numbers 32 and 33 in the Appendix which had positive responses between 50% and 60% were not judged feasible and relevant in a previous study2. Extension of this finding to the present study would justify the exclusion of all the practice standards with positive responses below 60% (marked with asterisk [*] in the Appendix) from standards that can be recommended for use in Benin City, and in fact, Nigeria. The proximity of the 60% to the mean positive responses when compared with 50% further justifies the need for the exclusion. Thus, only the 47 standards in the Appendix without asterisk are being recommended for initial application in Benin City. Studies by Desselle and Rappaport2 on the initial 52 practice standards suggested by the Delphi Expert Panel indicated that only 43 of the standards were rated positively for feasibility and 50 of them were rated positive for relevance. The differences between some of the standards being identified in this study and those previously identified are not unexpected as pharmaceutical care is at its infancy in Nigeria. Nevertheless, the similarity of most of the positively rated standards in the previous study2 to the 47 standards being recommended in this study is remarkable and supports the reliability of the outcome of this present study. Clearly, an adequate pharmaceutical service provided by pharmacists is a vital component of Primary Health Care. This is recognized by World Health Organization (WHO), and several publications emphasize the important role of the pharmacist in health care delivery16-18. A previous study19 has shown that pharmacists are generally positive about trying to provide pharmaceutical care but possess moderate to high intentions to apply the standards. Lack of workable strategies to adopt pharmaceutical care has been suggested as a possible reason for poor response on intention to apply the standards by many pharmacists19. The low positive response to current application and intention to apply the suggested standards in Benin City is contrary to report from the Netherlands where it is obvious that the pharmacists engage in many pharmaceutical care activities including health promotion and disease prevention, patient counseling and communication with other health professionals20. The current low application and intention to apply the practice standards in hospitals and community pharmacies is predictable. Pharmacists in Benin City, and in fact, most other parts of Nigeria, still practice in health care environments where there are little or no spaces provided for patient counseling. The medical profession has recently become hostile with the concept of clinical practice by pharmacists. Also, most of the pharmacists frequently demonstrate lack of confidence and assertiveness needed to effectively carry out their clinical roles in hospitals. Furthermore, the provision of pharmaceutical care is not merely a function of individual decision-making but is strongly impacted by pharmacists' perceived control over their practice environments21. These facts may 62 account for the low positive response on current application and intention to apply the pharmaceutical care standards. This calls for urgent attention by the Pharmaceutical Society of Nigeria, the Pharmacists Council of Nigeria (the regulatory organ of the practice of pharmacy in Nigeria) and all pharmacists practicing in Nigeria, to seriously address the needs of patients, and better health care for them through effective pharmaceutical services. The pharmacists in Nigeria should be made aware of this obligation. Challenges posed by the low positive responses on the current application and intention to apply each of the standards demand an early development and implementation of guidelines and standards for pharmaceutical care in Nigeria. Few pharmacists who currently apply some of the practice standards had clinical pharmacy training and work in hospitals and community pharmacies. The use of the suggested 52 practice standards in this study may have introduced bias as suggested in previous reports22-24. Nevertheless, many pharmacists in Benin City, and indeed Nigeria, are still not familiar with expected standards of practice of pharmaceutical care. This justifies the use of the known suggested practice standards. CONCLUSION In addition to known factors affecting the implementation of pharmaceutical care in many countries (such as USA and Australia), the lack of pharmaceutical care practice standards applicable in Benin City, and in fact in Nigeria, is a major barrier to the implementation of pharmaceutical care in Nigeria. Pharmaceutical care practice standards that can be effectively applied in improving effective pharmaceutical services in Benin City have been identified. The identified 47 standards are most likely to stimulate the widespread implementation of pharmaceutical care in Nigeria if seriously addressed by the Pharmacists' Council of Nigeria, the Pharmaceutical Society of Nigeria and Nigeria pharmacists. Implementation of these standards will enable the patients and health care professionals to appreciate the value of the pharmaceutical care services in optimizing therapeutic and economic outcomes. The process of adopting innovation typically has several, significant stages of development and testing prior to adoption20. Thus, further studies would be needed to appraise and evaluate the standards with the aim of categorizing and simplifying them. This will hopefully provide a logical validity instrument to measure performance. ACKNOWLEDGEMENTS The authors are grateful to all the pharmacists who participated in this study. APPENDIX The Fifty-Two Suggested Practice Standards Obtained From the Round One Delphi Procedure2 1. The pharmacist shall devise a standard system of data collection of all necessary medical and
personal information from each patient, including: prescribing physician(s), medication history,
medical condition & diagnoses, allergies, and other data that would assist in detecting potential
medical or drug-related problems. REFERENCES 1. Hepler CD, Strand LM. Opportunities and
responsibilities in pharmaceutical care. Am J
Hosp Pharm 1990; 47: 533-43. Full text of this journal is also available online at http://www.tjpr.freehosting.net © 2003 - Pharmacotherapy Group, Faculty of Pharmacy, University of Benin, Benin City, Nigeria. The following images related to this document are available:Photo images[pr02009t4.jpg] [pr02009t3.jpg] [pr02009t2.jpg] [pr02009t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}