 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
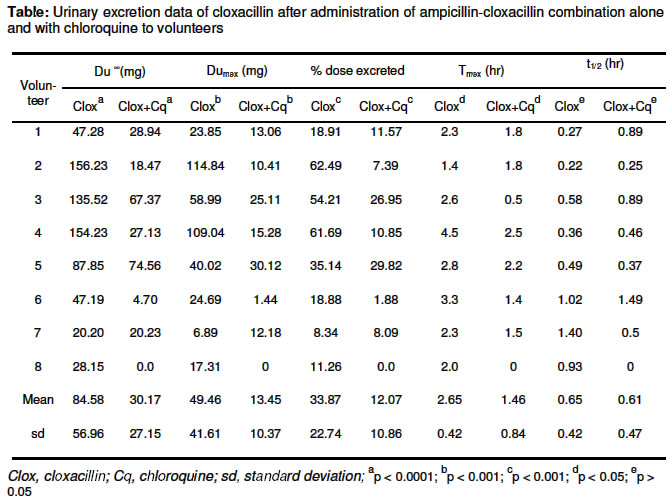
Tropical Journal of Pharmaceutical Research , Vol. 2, No. 1, June, 2003 pp. 169-173 Research Article Chloroquine reduces urinary excretion of cloxacillin when it is administered concurrently with ampicillin-cloxacillin combination Chinedum P. BabalolaΦ, Titilayo T. Fashedemi and Ajibola A. Olaniyi Department of Pharmaceutical Chemistry, Faculty of Pharmacy, University of Ibadan, Nigeria Code Number: pr03007 Abstract Purpose: To investigate a possible effect of chloroquine on urinary excretion of cloxacillin when chloroquine is administered concurrently with ampicillin-cloxacillin combination. Key words: Drug-drug interaction, bioavailability, chloroquine, cloxacillin Introduction It is common for patients with multiple medical problems to be taking many drugs concomitantly1. It is also becoming increasingly obvious to physicians and other members of the health-care team that many drug combinations when used inappropriately have the inherent potential to interact adversely2. The co-administration of antibiotics and antimalarial agents is common in the tropics as a result of frequent association of malaria with other infections such as respiratory tract infections, urinary tract infections and diarrhoea3. Earlier studies4, 5 revealed that the bioavailability of ampicillin and cloxacillin (β-lactam antibiotics) is significantly reduced following oral co-administration with either chloroquine or proguanil both of which are antimalarial drugs. Chloroquine is widely used for the treatment and prophylaxis of falciparum malaria as well as for rheumatoid arthritis5. The combination of ampicillin and cloxacillin produces a broad spectrum antibiotic activity against both Gram positive and Gram negative bacteria. Specifically, cloxacillin is a penicillinase-resistant and acid-stable penicillin used for the treatment of infections caused by penicillinase producing Staphylococci and Pneumococci. In combination with ampicillin, it is available as Ampiclox® (SmithKline Beecham, Lagos, Nigeria) and other generic forms6. In 1985, Ali4 investigated the interaction between chloroquine and ampicillin in ampicillin-cloxacillin administered orally. Ali's study did not evaluate the effect of chloroquine on cloxacillin bioavailability and there is currently no information on possible interaction of chloroquine with cloxacillin in ampicillin-cloxacillin combination. In this study, therefore, the effect of chloroquine on the urinary excretion of cloxacillin when chloroquine is administered concurrently with ampicillin-cloxacillin combination is evaluated. Materials and Methods Twelve healthy volunteers were recruited for this study but only eight of the volunteers complied fully with the protocol for the study and were included in the data presented. The eight volunteers included 6 males and 2 females aged between 21 and 30 years (mean, 25.3 ± 3.2 years), and weighing between 51 and 69 kg (mean, 61 ± 5.7 kg). The continuation of the study with the eight volunteers is supported by recent kinetic studies that have reported limited number of subjects6, 7, 8. Consent was obtained from each volunteer after full explanation of the protocol. The study protocol was approved by the Joint Ethics Committee of University of Ibadan/University College Hospital (UI/UCH) Ibadan, Nigeria. The study was a simple cross-over design in which the volunteers were not on regular medication, abstained from drugs two weeks prior to the administration of the study drugs, and throughout the duration of the study. The volunteers observed an overnight fast and were in fasting state till four hr after receiving the drugs, after which food was given to them. On the day of the study, each subject received a single oral dose of 500 mg of Ampiclox® capsules (SmithKline Beecham, Lagos, Nigeria, Batch No. 007) comprising of 250 mg cloxacillin and 250 mg ampicillin with a glass of water (250 ml). The subjects were allowed to take water ad libium after drug administration. Total urine voided was collected prior to and at 0-1, 1-2, 2-3, 3-5, 57 and 7-9 hr after drug administration. The volume of urine voided at each time interval was measured and recorded. An aliquot (30 ml) was stored in sample bottles. After a washout period of one week, 500 mg Ampiclox® and 600 mg chloroquine phosphate capsules (Capquin® from Evans Medical PLC, Lagos, Nigeria; Batch No. 009) were given concurrently with a glass of water (250 ml). Total urine voided was collected as stated above. The pH of all samples were taken and then stored at - 20 oC until analysis. Both the Ampiclox® and chloroquine capsules used in the study were subjected to pharmaceutical assessment including identification test, weight uniformity, and chemical assay following British Pharmacopoeia (BP) standards9, and were confirmed to meet the BP standards before they were used for this study. The urine samples were analysed for cloxacillin by a reversed-phase HPLC method using a modified method described by Treare et al. 10 and Abuirje et al. 11. An internal standard, dicloxacillin was used in the determination of the amount of cloxacillin in the various urine samples. Briefly stated, 200 µl of the urine was diluted to 1 ml with distilled water. The diluted urine sample (0.5 ml) was mixed with 0.1 ml of 10 µg/ml solution of the internal standard and made up to 1 ml with mobile phase consisting of methanol and 0.04 M sodium phosphate buffer, pH 4.5 (4.1:5.9). This was mixed in a vortex mixer for 20 sec., centrifuged at 3000 rpm for 3 min and 20 µl of the supernatant injected onto the HPLC column (RP-8, 10cm x 4 mm) at a flow rate of 0.7 ml/min. Detection of cloxacillin was achieved with a UV detector at a wavelength of 225 nm. The between-day and within-day coefficient of variation (CV%) were assessed and found to vary between 2 and 10 % while the recovery was determined to be 99%. From the data obtained, the amount of unchanged drug (cloxacillin) excreted was determined for each subject. Pharmacokinetic parameters (maximum peak of excretion [Dumax], time of maximum peak excretion [Tmax], total amount excreted unchanged [Du∞], % dose excreted and elimination half-life [t1/2]) were evaluated according to standard methods12. Results were recorded as mean ± SD. Statistical comparison of data was achieved using the paired Student's T-test and F-test. At 95% confidence interval, any 2-tailed p-value less than 0.05 was considered significant. Results The chloroquine and Ampiclox® administered were well tolerated by the volunteers. However, one of the volunteers experienced reversible dizziness, visual disturbance and itching when chloroquine was administered while another volunteer experienced itching and rashes after intake of Ampiclox® alone and later withdrew from the study. The data for these latter volunteers were excluded from the data of the eight volunteers presented. Details of the pharmacokinetic parameters obtained from urine are shown in the Table. There were wide inter-and intra-individual variations in the excretion results obtained. The co-administration of chloroquine and Ampiclox® produced significant decrease (p < 0.0001) in Du∞, Dumax, % excreted and max. of cloxacillin. Total amount of cloxacillin excreted decreased in seven of the eight subjects and this included a subject who had no cloxacillin in the urine. Up to 64% decrease in the mean cloxacillin content in urine was produced by the chloroquine (p < 0.0001). The Tmax was significantly reduced by 45 % (p < 0.05). However, the t1/2 of cloxacillin was not significantly (p > 0.05) affected by the concurrent administration of chloroquine and Ampiclox®. Discussion Cloxacillin is rapidly but incompletely (30% - 80%) absorbed from the gastrointestinal 13, 14. It is bound to plasma protein to a great extent (about 94%), metabolized to limited extent and excreted unchanged in urine by glomerular filtration and renal tubular secretion13,14 . The present study shows that chloroquine tremendously reduces the excretion of cloxacillin in urine in Ampiclox®. The excretion of cloxacillin when Ampiclox® was taken alone was determined to be approximately 3 times the amount when Ampiclox® was taken together with chloroquine. The mean percentage of cloxacillin excreted in urine (34%) when Ampiclox® was administered alone was similar to that of earlier reports13. In the presence of chloroquine, the reduction in urinary excretion of cloxacillin (mean, 64.4%) suggests significant interaction between chloroquine and cloxacillin. The wide inter-and intra-individual variations in the urinary data presented can be explained on the basis of erratic nature of drug excretion in urine, which is also related to pH changes15. Although urine sampling is one of the noninvasive methods of drug level monitoring and can be convenient for pharmacokinetic studies especially for drugs that are excreted in urine in appreciable quantities such as cloxacillin 15,16, it may be difficult to conclude that chloroquine reduces the bioavailability of cloxacillin in ampicillin-cloxacillin combination unless plasma level data are available for comparison. Chloroquine may have led to a reduction in plasma levels of the cloxacillin in the presence of chloroquine by enhancing the degradation of cloxacillin or reducing the absorption. Further studies are needed to confirm such possibilities. Whether there is increase or decrease in plasma concentration of cloxacillin as a result of concurrent administration with chloroquine, the therapeutic implication is evident. Ali4 has earlier reported about 35 % reduction in urinary excretion of ampicillin by chloroquine when taken concurrently in seven volunteers, but the Tmax of excretion remained unchanged. In a similar study carried out in our laboratory5, proguanil reduced the urinary excretion of cloxacillin by about 50 % but the Tmax and t1/2 were not significantly affected. The effect of chloroquine on both the rate and extent of excretion of cloxacillin observed in the present study is more pronounced than the earlier studies. Unfortunately, the mechanism of this interaction is still unknown. Though without proof, Ali4 attributed the chloroquine interaction with ampicillin to possible slowing of gastric motility and enhancement of gut motility. It may also be possible that these antimalarials being basic could be forming complexes with these betalactam penicillins thereby reducing absorption. Chloroquine is reported to exhibit antispasmolytic properties similar to papaverine, thus leading to inhibition of gastric motility17, 18. Such reduction in gastric motility may lead to acid hydrolysis of these penicillins. Further studies will be conducted to confirm whether there is reduction in the bioavailability of cloxacillin by the chloroquine, and to determine the mechanism of this chloroquine-cloxacillin interaction. Conclusion The concurrent administration of chloroquine and ampicillin-cloxacillin combination leads to an interaction between the chloroquine and cloxacillin. This interaction results in significant reduction of urinary excretion of cloxacillin. Whether this interaction results in the reduction of the bioavailability of cloxacillin is as yet to clear. However, there is therapeutic implication. Thus, caution should be exercised when prescribing or administering chloroquine and cloxacillin for concurrent administration. If they must be administered to a patient, it may be essential to administer the two drugs separately. Acknowledgement The authors thank Mopson Pharmaceuticals Ltd, Lagos for providing the HPLC used for the analysis. References
Full text of this journal is also available online at http://www.tjpr.freehosting.net © Pharmacotherapy Group, Faculty of Pharmacy, University of Benin, Benin City, Nigeria. The following images related to this document are available:Photo images[pr03007t1.jpg] |
| |||||||||

{kind=link}