 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Tropical Journal of Pharmaceutical Research , Vol. 2, No. 1, June, 2003 pp. 175-182 Research Article Prescribing practices in two health care facilities in Warri, Southern Nigeria: A comparative study Patrick O ErahΦ, GO Olumide and Augustine O Okhamafe Pharmacotherapy Group, Faculty of Pharmacy, University of Benin, Benin City,
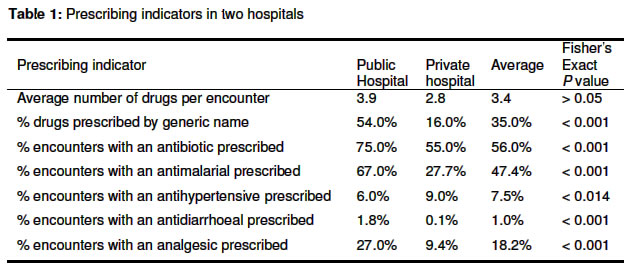
Nigeria Code Number: pr03008 Abstract Purpose: Inappropriate prescribing has been identified in many health facilities in developing countries. The purpose of this study was to evaluate the prescribing practices in two health care facilities in Warri located in south-south geopolitical region of Nigeria and identify factors influencing the practices. Keywords: Drug prescribing, Indicators, Practices, Southern Nigeria Introduction A quarter of the world's population is concentrated in developing countries and has access to only a small proportion of the world's drug production1. Health budgets in the countries are generally small, when compared to developed countries, and 3040% of the total health budget is spent on drugs2. Considering the small amount of funds available for drugs in these poor countries, it is desirable to prescribe drugs rationally for optimal benefit to the patients. However, field surveys carried out in many of these countries have highlighted a significant degree of inappropriate use of drugs in their health care facilities3. Studies by Hogerzeil and his colleagues, and in Nigeria, have shown that there is a high rate of polypharmacy, overuse of antibiotics and injections and use of drugs with unproven efficacy4-7. Inappropriate prescribing is known all over the world as a major problem of health care delivery; in Nigeria, this has compounded the efficient and ever increasing cost of health care delivery. The importance of patients' involvement in prescribing practices has being recognized8,9. Many patients taking drugs for chronic diseases are actively involved in decisions about their drugs rather than being passive recipients of medical care10, 11. However, the role of the prescriber is critical, as he has to take decision on the use of drugs in a disease situation. Consultation with a clinician by a patient involves understanding the patient, finding common ground regarding management (partnership), and enhancing the clinician-patient relationship12. Seeking the prescribers' opinion on their prescribing practices is essential, as their habits and many features of their practice environments influence their abilities to use drugs appropriately. Although various factors are known to affect prescribing practices, the most important factors are frequently assumed in many health facilities in Nigeria9, 12, 13. The assessment of the existing prescribing practices in a health facility helps to identify the specific drug use problems, which need to be understood before any meaningful intervention can take place. In this study, we evaluated drug prescribing practices in two health care facilities in south-south geopolitical region in Nigeria providing mainly primary and secondary health care using the WHO Prescribing Indicators. We highlighted problems in drug usage in the health care facilities, and useful recommendations that can improve drug prescribing practices in Nigeria were proffered. Methods SettingThis study was carried out in two health care facilities in Warri, Delta State in Southern Nigeria. Warri is an urban area with a population of over 1 million multi-ethnic inhabitants. The major economic activity in the area (providing accommodation for the regional headquarters of many local and multinational oil companies) is oil exploration. Available health care facilities in the area include a tertiary health care centre, hospitals, and medical and diagnostic clinics. In addition, there are many pharmacies, patent medicine stores and traditional herbal homes serving as first point of call for health seekers in the communities. However, we selected a 250-bed public (government owned) Central Hospital and a 50-bed private hospital in the area for this study. These facilities, providing mainly primary and secondary health care services for the communities, were selected because each of them had an outpatient department with an annual attendance of over 40,000 patients. Medical care was provided by 10 -32 clinicians with 2 - 20 years post-qualification experience. The number of clinicians in each of these hospitals was the highest in any of the health care facilities in the area and was considered suitable for the assessment of factors affecting prescribing practices. Drugs prescribed in each of the facilities were usually dispensed in the hospital pharmacy and where the drugs were not available, patients were advised by the pharmacists to purchase their drugs from private pharmacies. As in other public hospitals in Nigeria, patients pay for drugs supplied to them by the hospital pharmacy in Central Hospital, unlike the private hospital where drugs were supplied free of charge. Records of prescriptions were properly stored in the health facilities and readily available for the evaluation of drug usage. Drug prescribing pattern Prior to this study, we obtained ethical approval for the protocol from the Delta State Ministry of Health. The data for this study were collected from records kept in the outpatients departments of the health facilities studied. Prescription records (1000) from January to December 2000 were obtained retrospectively from each of the hospitals by systematic sampling as earlier reported7. For easy accessibility to data, we included records of all patients who were 12 years old and above but excluded records of antenatal and post-natal clinic attendances. We applied the WHO Prescribing Indicators in evaluating the prescribing pattern in the health facilities as described in the How to Investigate Drug Use in Health Facilities: Selected Drug Use Indicators12. Information was obtained using the Prescribing Indicator Form12. The following WHO Core Prescribing Indicators (A-C) and disease specific prescribing indicators (D-G) were evaluated:
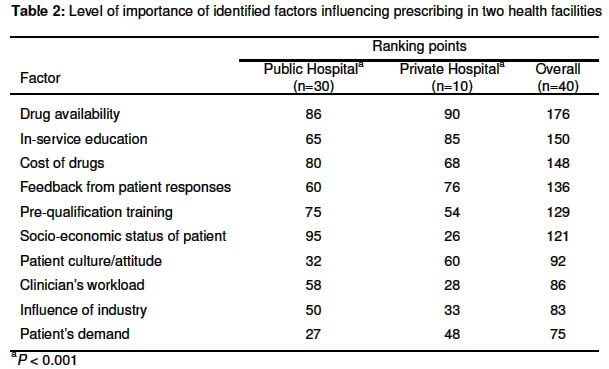
Factors contributing to prescribing practices Following informal interviews with 10 prescribers (5 - 20 years post-qualification experience) in each of the two hospitals, we identified ten factors considered to be contributing mainly to prescribing practices in the hospitals, some of which have been identified elsewhere (see results)14-18. In order to have a better understanding of these factors, we decided to rank them in order of importance, from the prescribers' perspectives, by using a one-page pretested and self-administered questionnaire distributed to 10 prescribers in the private hospital and 30 prescribers in the Central Hospital. These prescribers were involved in prescribing in the outpatients departments in the hospitals. In addition to providing information on demography, qualification, type of training received and years of professional experience, the questionnaire made provision for the ranking of the factors identified in the informal interview, in accordance with the clinicians' perceived level of contribution to the prescribing practices in the hospitals where they were working. For this purpose, a ranking scale of 0 to 10 was adopted where a score of 0 indicates that the factor had no contribution, a score of 1 represents the lowest contributing factor and a score of 10 represents the highest contributing factor. Analysis of data All data collected were entered into a computer spreadsheet, Microsoft Excel (Microsoft Corporation, USA) and double-checked before calculations were done. Computations on drug usage pattern were carried out as earlier described12. Following literature review, we compared the Core Prescribing Indicators data from this study with those obtained in previous similar studies in developing and transitional 3, 12, 19-22. In evaluating the level of importance of the factors influencing prescribing, the scores assigned by the questionnaire respondents to each factor were added to arrive at the overall ranking. Comparison of data was accomplished using Chi-square test or Fisher's exact test (for small data comparison) at a confidence interval of 95%. Two-tailed P values less than or equal to 0.05 were considered significant. Results Drug prescribing pattern Two thousand prescriptions (100%) were successfully evaluated. Prescribing indicators in the two hospitals are shown in Table 1. Average numbers of drugs per encounter in the health facilities were not significantly different from each other (P > 0.05). The average number of the two hospitals (3.4) was similar to those of Indonesia and Nigeria obtained in a previous study in 1993 but higher than the average obtained from similar studies conducted in a number of developing and transitional 3, 12, 19-22. The percen-tage of drugs prescribed by generic name and the percentage of encounters with an antibiotic prescribed in the private hospital were significantly lower than those in the public hospital (P < 0.001). Unlike the data from the public hospital, we found a significant difference between the percentage of drugs prescribed by generic name in the private hospital when compared with the average of those obtained from similar studies conducted in a number of developing and transitional countries (P < 0.001). The percentage of drugs prescribed by generic name in the public hospital was similar to the percentage reported in a previous study in Nigeria12. However, unlike the private hospital, the percentage of encounters with an antibiotic prescribed in the public hospital was significantly higher than that reported previously in Nigeria or the average of those reported in developing and transitional countries3, 12, 19-22. Encounters with antimalarial and analgesic drugs in the private hospital were more than twice the encounters in the public hospital (P < 0.01). The encounters with antidiarrhoeal drugs in the private hospital was as much as eighteen times that in the public hospital (P < 0.001). However, the percentage encounters with antihypertensive drugs were significantly higher in the private hospital than in the public hospital (P = 0.014). Factors influencing prescribing The questionnaires distributed to the 40 clinicians were received, giving a response rate of 100%. During the informal interview with the clinicians in the health facilities, the ten factors identified to be contributing factors to prescribing practices were patients' factors (demand, culture/attitude and socio-economic status), prescribers' factors (pre-qualification training, in-service education, workload and feedback from patient responses), drug factors (availability and cost) and influence of industry (medical detailing). After ranking these factors in order of importance (Table 2), we found a significant difference between the two health facilities (P < 0.05). The factors were found to be in the following order of importance by the clinicians in the public hospital: socioeconomic status of patient, drug availability, cost of drugs, pre-qualification training, in-service education, feedback from patient responses, clinician's workload, influence of industry, patient culture/attitude and patient's demand. In the private hospital, the order of importance as observed by the clinicians was in the following order: drug availability, in-service education, feedback from patient responses, cost of drugs, patient culture/attitude, pre-qualification training, patient's demand, influence of industry, clinician's workload, and socio-economic status of patient. Discussion Drug prescribing pattern A prescription provides an insight into a prescriber's attitude to the disease being treated and the nature of health care delivery system in the community23. This study has provided a better understanding of the prescribing practices in the health care facilities studied and strategies for intervention. Poor quality of pharmacotherapy is reflected in the results presented and may be indicative of poor financing of health24. The polypharmacy observed in the data and continual inappropriate prescribing practices in the health facilities can increase the chances for non-compliance and side effects or drug interactions25. Increasing generic prescribing could substantially reduce the cost of drugs for the patients, and reduce cost for pharmacies25, 26. However, we observed low frequencies of generic drug prescribing in the two health facilities particularly when our results were compared with those reported in Zimbabwe (94%) and Tanzania (82%)27, 28. The similarity of the frequency of generic prescribing in the public hospital and the frequency in an earlier national survey is an indication that the prescribing habits of the clinicians in the public hospital need to be addressed. Generic prescribing can be enhanced by restriction or total elimination of drug samples often given to clinicians to influence their decision on prescription of drugs29. Inappropriate use of antibiotics can potentially lead to antimicrobial resistance and increase the necessity to use more expensive antibiotics to treat life-threatening infections30-32. In Nigeria, antibiotics usage is largely uncontrolled and probably accounts for widespread resistance33. Interestingly, antidiarrhoeal usage in these facilities was mainly in the form of antibiotics and not oral rehydration therapy, which raised the question of the appropriateness of the use of such drugs. However, it was not possible, from the approach we adopted, to establish whether the use of antibiotics in this study was inappropriate, as further studies involving laboratory and/or clinical data would be needed. However, antibiotics usage in the health facilities may have been inappropriate as observed in previous studies34, 35. The use of antimalarial drugs in both facilities was significantly different (P < 0.05) from the 49.3% reported by Isah and coworkers in a similar study in Benin City in 19977. Malaria is endemic in Warri and the frequency of prescription of antimalarial is expectedly one of the highest encounters. The significantly higher usage of antihypertensive drugs in the private hospital when compared with the public hospital reflected a higher number of patients presenting with hypertension in the private hospital which may be due to early detection in the private hospital. We found a significantly lower rate (P < 0.05) of analgesic use in this study in comparison with an earlier study in Benin City, Nigeria where 72.3% of the encounters had an analgesic drug prescribed7. We are constrained to assume that the almost threefold rate of prescription of analgesics in the public hospital when compared with the private hospital is influenced by patients' demand, which was identified as a factor influencing prescribing practices by the clinicians in the informal interview. We did not encounter the prescription of any drug withdrawn by the manufacturer, as was the case in the study carried out in Uzbekistan25. Factors influencing prescribing We observed divergence of opinions on the factors that influence prescribing in the two health facilities and these appear to be influenced by the practice environments. Drug availability was either first or second top consideration in prescribing in both facilities; developing countries are known to have problems of accessibility to drugs1. Socioeconomic status was viewed to be the second most important factor influencing prescribing practices in the public hospital whereas in-service education was seen as the second most important factor in the private hospital. The ability of the ordinary (poor) patient to purchase needed drugs depends on the patient's socio-economic status - a factor known to influence selfmedication36. It was interesting that the clinicians in the private hospital rated socioeconomic status 9th. An explanation for this finding can be deduced from the fact that drugs were provided free of charge to patients in the private hospital. Patients' inability to purchase their drugs because they cannot afford to pay the cost is a common occurrence in Nigeria hospitals. Several reports have described the important role of pharmaceutical advertising and marketing on prescribing habits14, 16, 37. The elimination of gifts from the pharmaceutical industry can improve prescribing habits by clinicians38, 39. However, the low rating of the influence of industry by the clinicians in both hospitals is predictable from the reduced aggressive marketing strategies of pharmaceutical companies in Nigeria due to the difficult economic situation. Despite the recognition of the importance of patients' involvement in health care in medical practice and hence the need to be identified and addressed, patients' demand was also not highly rated by the clinicians8, 40. This calls for clinicians to always involve patients in their prescribing decisions for effective drug management of disease states. Limitations of the study The findings of this study present a clear understanding of the prescribing practices in some health facilities in Nigeria. Despite the usefulness of our data, the study is limited by the absence of data on percentage of encounters with prescribed injections and percentage of drugs prescribed from essential drugs list (EDL) or formulary and the small number of clinicians involved in the feedback study. Nevertheless, we are convinced that the data presented provides useful information on the prescribing practices in the health facilities studied. Our results serve as baseline data for further nationwide studies on the prescribing practices with the hope of applying effective interventions to reverse inappropriate use of drugs. Conclusion This study has documented polypharmacy, overuse of antibiotics and low rate in the use of generic drugs, particularly in a private hospital. The overuse of drugs is significantly lower in the private hospital than in the public hospital investigated. Major factors responsible for prescribing practices in the two health facilities studied in Warri include drug availability, training of clinicians, cost of drugs, feedback from patients and socioeconomic status of patients. Interventional strategies that can be applied to improve the prescribing practices include feedback from pharmacy, jointly developed policy on prescribing, re-training of clinicians and prescription control14-18. It is essential to extend this study to other health facilities across the country. Acknowledgement We are grateful to the management and other staff of both Central Hospital and Shell Petroleum Development Company Hospital, Warri, Delta State, Nigeria. References
Full text of this journal is also available online at http://www.tjpr.freehosting.net © Pharmacotherapy Group, Faculty of Pharmacy, University of Benin, Benin City, Nigeria. The following images related to this document are available:Photo images[pr03008t1.jpg] [pr03008t2.jpg] |
| |||||||||

{kind=link}
{kind=link}