 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
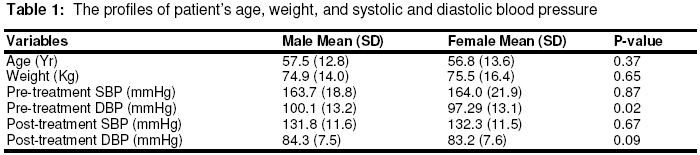
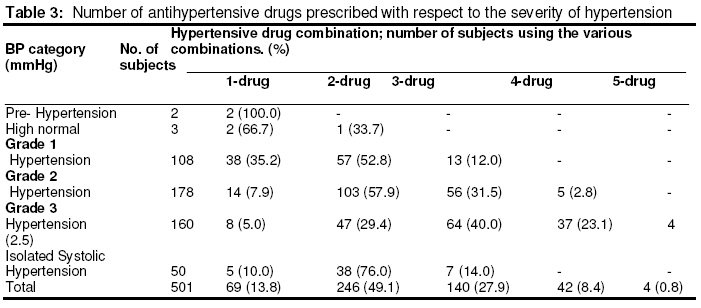
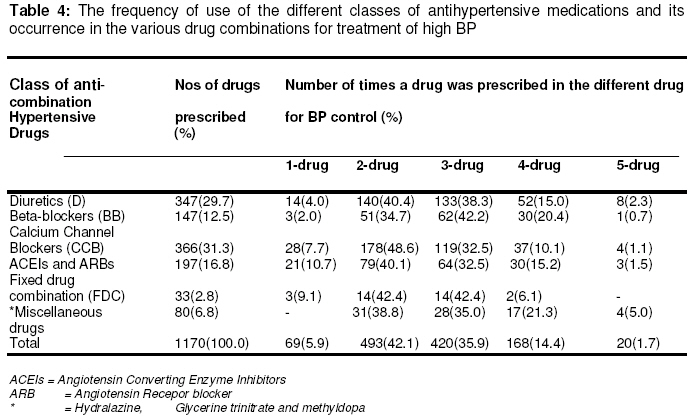
Tropical Journal of Pharmaceutical Research, Vol. 7, No. 2, June 2008, pp. 945-952 Research Article Adherence to International Guidelines in the Management of Hypertension in a Tertiary Hospital in Nigeria VU Odili*1, EK Oghagbon2, NA Ugwa3, UM Ochei1, and OE Aghomo1 1 Dept. Of Clinical Pharmacy & Pharmacy Practice, Faculty of Pharmacy, University of Benin, Benin City, Nigeria, Code Number: pr08012 Abstract Purpose: The role of physicians in the overall management of hypertension and their adherence to the JNC VII, WHO/ISH and ESH guidelines were examined in this study. Keywords: Adherence, Guidelines, Hypertension, Management. INTRODUCTION Hypertension is considered a public health problem in sub-Saharan Africa, as it is increasing in importance as a major cause of cardiovascular disability and mortality1 . The world over, treatment of hypertension has been demonstrated to be beneficial to the patients, yet the levels of control of blood pressure (BP) in sub-Saharan Africa is low. A Nigeria report, indicates that only 25.4% of patients attending a hypertensive clinic in a tertiary hospital achieved an optimum BP set at <140/90mmHg1 . The need to improve the global control of high BP has necessitated the stipulation of various hypertension classification and treatment guidelines. In recent times, it includes those of World Health Organization/International Society of hypertension (WHO/ISH)2 The Sixth and Seventh reports of the Joint National Committee on the Prevention, Detection, Evaluation and Treatment of Hypertension (JNC VI and JNC VII.)3,4 guidelines. Practice guidelines serve as useful tools for clinical decision making. They also help to reduce the variation in practice, guide appropriateness and measure quality of care. Many factors thought to be responsible for poor BP control in Africans have been evaluated, but the extent of adherence to treatment guidelines by key health care players such as doctors in the management of hypertension5 is yet to be ascertained in this environment. In places were similar studies have been done, reports showed divergent views on the influence of the guidelines on prescription patterns of doctors6 . This study aims to assess the extent of adherence of physicians in this environment to recently updated international guidelines in the management of hypertension. METHODS This retrospective study was carried out at University of Benin Teaching Hospital, Benin City, Nigeria. The first step was to retrieve the case notes of patients that attended the consultant out-patients’ clinics between September and November 2005, from the Medical Records Unit of the hospital. The case notes of patients who were first diagnosed to be hypertensive between 1 January 2004 and 30 September 2005 were selected. Also selected were those previously diagnosed to be hypertensive, but defaulted from clinic attendance for at least one year were included only if they represented in the clinics during the period under consideration. This period (1 January 2004 to 30 September 2005) was chosen because the JNC VII, European Society for Hypertension Guidelines7 and updated WHO/ISH Guidelines8 , came into focus in 2003. All the case notes of patients who met the inclusion criteria and who were booked for their regular appointment during the study period were included. A total of 501 case notes of patients were selected and from them the following information were retrieved; age, gender, body weight, occupation, BP reading (systolic blood pressure; SBP and diastolic blood pressure; DBP) at diagnosis and last clinic attendance, and the pattern of prescribed drugs for hypertension. In examining the prescribed drugs, attention was paid to whether the patient was on monotherapy or multitherapy. Multitherapy was defined as two or more drug combinations from different antihypertensive drug classes. Antihypertensive classes in the study included thiazide diuretics (D), betablockers (BB), calcium channel blockers (CCB), angiotensin converting enzyme inhibitors (ACEIs), angiotensin receptor blockers (ARBs). The pattern of drug combination was also examined. The number of drug combinations in relation to increases in BP was noted. These were all reviewed against the recommendations of the treatment guidelines. According to JNC WHO/ISH and ESH guidelines, effective drug combinations include; (I) D and BB. (II) D and ACEI/ARB. (III) CCB and BB. (IV) CCB and ACEI or ARB. (V) CCB and D. (VI) alpha–blocker and BB. (VII) Other combinations (e.g. with centrally acting agents, including alpha 2-adrenoceptor agonist and imidazoline-I2 receptor modulators, or ACEIs or ARBs) can be used, if necessary. (VIII) In many cases, 3 or drugs may be necessary. The BP profiles of the patients were also graded based on the above mentioned guidelines, i.e. prehypertension, high normal, grade 1, 2, hypertension and isolated systolic hypertension. 3,4 Subjects with co-morbidities were noted and the number of co-morbid conditions was reported as different disease entity. For example, the number of patients with diabetes mellitus, congestive heart failure et cetera was reported individually. Data collected were analysed using SPSS 10.0 for Windows. The means of continuous variables (age, SBP, DBP, weight) were compared using Student t-test, with the level of significance set at P < 0.05. Categorical variables such as number of drug combinations in relation to increases in BP and the number of patients in the various BP categories were reported as simple percentage frequency. RESULTS Out of the 501 patients selected in line with set criteria, 60% of them were females, while 40% were males. The mean diagnostic SBP for males was 163.7 mmHg ± 18.8 and 164.0mmHg ± 21.9 for females. The difference was not significant (P>0.05). However, the males had significantly higher mean DBP (100.1 mmHg ± 13.2) than females (97.3 mmHg ± 13.1) (P < 0.05).There was a significant reduction in systolic and diastolic blood pressures in all subjects (P< 0.05) after commencement of treatment. However, this difference was not reflected between genders; the mean SBP and DBP after commencement of treatment in the males was (SBP; 131.8mmHg ± 11.6, DBP; 84.3mmHg ± 7.5) and females (SBP; 132.3mmHg ± 11.5, DBP; 83.2mmHg ± 7.6). (Table 1) Based on the JNC VII classification a greater percentage of the patients (35.5%) belonged to the grade 2 hypertension category while the pre-hypertension class had the least (0.4%). When combined, patients in grade 2 and 3 hypertension categories made up 67.5% of the study population. (Table 2). The prevalence of co-morbid condition increased with the severity of hypertension. It increased from 0.9% in pre-hypertension to 33.7% in grade 2 and grade 3 classes, respectively (Table 2). Diabetes mellitus (17.6%) was the commonest co-morbid condition followed by cardiovascular diseases (coronary heart disease, angina pectoris, myocardial infarction, 4.4% and congestive heart failure 3.4%. (Figure 1.) A combination of two anti-hypertensive medications was found to be most commonly used in the management of grades 1 and 2 hypertension. Furthermore, it was also found that the number of drugs prescribed for patients increased with the severity of the disease As shown in Table 3, three-drug multitherapy was used in 12.0% of grade 1 hypertensive subjects, 31.5% of grade 2 and 40.0% of grade 3. In the same vein, 4 drugs were used in 2.8% of grade 2 cases and 23.1% of grade 3 (Table 3). A wide variety of anti-hypertensive medications were used in this centre (Table 4). The most commonly prescribed drug was CCB (31.3%), and this was followed by diuretics (29.7%). In those on monotherapy and two drug multitherapy, CCBs were the most commonly prescribed antihypertensives a as it made up 40.6% and 36.2% of the drugs in the respective combinations (Table 4). But in drug combinations that had three or more drugs diuretics were the most frequently prescribed agents (3-drugs; 31.7%, 4-drugs; 31.0%, 5-drugs; 40.0%). Calcium channel blockers plus diuretics was the commonest 2drug combination (36.6%), followed by CCB plus ACEI (19.5%) and CCB plus BB (11.4%). In the 3-drug combination, CCB plus diuretic plus BB was found in 32.9% of cases and this was closely followed by CCB plus diuretic plus ACEI (31.43%). The most frequent drug combination pattern in this centre was CCB plus diuretic (2-drugs group), CCB plus diuretic plus BB (3-drugs group), and ACEI plus BB, plus CCB plus diuretic (4-drugs group). There was no prominent drug prescription pattern in the patients receiving a combination of 5 antihypertensive drugs. Methyldopa is still being used as an antihypertensive in this environment. This was particularly observed in the higher drug combinations, where it was a component of 4-drug combination to the extent of 33.3% and 50.0% in the 5-drug combinations. Patients in these two classes of multitherapy only made up 9.2% of the study population. DISCUSSION It was observed that there were a higher number of women than men encountered over the study period, Some workers have opined that this is either because males do not regularly keep clinic appointments9 , or it is a reflection of poorer awareness of BP status among them. In this study this fact seems reiterated by the observation of significantly higher mean pre-treatment DBP in men, despite a similar SBP in both sexes. Similar observation was noted elsewhere. (10, 11) Most patients presented to the hospital with a mean BP consistent with the grade 2 hypertension classification, this is similar to the finding of a study done in Ilorin, Nigeria12 .In about 68% of the study population the pretreatment BP classifications were in grade 2 and grade 3. This is disturbing especially with the observation that this group had the highest prevalence of co-morbidity. The authors were unable to ascertain how many of these subjects had a co-morbid condition at the time of their first visit. Treatment guidelines under focus emphasize the need to evaluate the total cardiovascular risk of patients before the commencement of drug treatment. It is advised therefore, that the evaluation of patients for possible co-morbidities should be emphasized in this environment giving their common late presentation. The subjects in the pre-hypertension and high normal groups, who were placed on drugs, were so treated probably because of the presence of comorbidities. This is in keeping with the treatment guidelines which states that the presence of co-morbidities in pre-hypertension and high normal BP necessitates the use of drugs. There was a ready recourse to the use of multitherapy in the subjects, as only 69 (13.8%) of them were on monotherapy. A study in India13 showed a common trend among patients attending a cardiology clinic, in which most of them were on multiple therapies with two combined antihypertensives. Like in the present study, this pattern is encouraged by the guidelines, which states that small doses of different classes of antihypertensive drug is more beneficial than a high dose of one. This advice probably accounts for 60% of antihypertensive drug visits in United States, getting polytherapy of three or more classes of drugs14 . The finding that CCB was most commonly prescribed drug in this study agrees with some other reports15 16 which were done outside Nigeria. This was not the case in a study done in Ibadan, Nigeria17 where thiazide was the most commonly prescribed antihypertensive. The Ibadan study which was published in 2003 may probably be influenced by the volume dependency of black hypertensives and the ALLHAT study 18 released in 2002. The ALLHAT study had emphasized the use of thiazide in its recommendations, and this has been reported to increase prescription pattern of the drug by physicians.19 The difference in the level of thiazide use in this study and the Ibadan’s, could not be due to the factor of co-morbidity, because the prevalence of diabetics in the other study was 22% as against 17.5% in Ibadan. The present preference for CCB could, among other factors, be due to the influence of the treatment guideline. The Ibadan study mentioned that prescription of CCB, was already experiencing an upward trend at that time. It was noted in Ibadan17 , that monotherapy on CCB achieved normotension (<140/90mmHg) better than diuretics. This claim is cautioned by the work of Wassertheil-Smoller et al20 which found that monotherapy with diuretic was equal or superior to others, in preventing CVD complications of high BP in women. Furthermore, it has been suggested that factors that should determine the use of thiazides are sex, age and co-morbidities21 . What this infers, is that in prescribing drugs for hypertension, the role of gender should be taken into consideration. In the present study, CCB plus diuretic combination was the commonest multitherapy. The same combination has been reported to have the best rate of BP control in one study.16 Similar to the earlier observation, this combination is said to be poor in women, as it has been associated with a higher risk of CVD mortality. 20 Other centres are in favour of the combination of CCB plus BB15 . We observed that, as the need for more classes of drug arose for BP control, the use of diuretic became more prominent. It was the commonest component of multitherapy in this study. This infers its usefulness in patients in this environment. According to the ESH guidelines, thiazides are useful in elderly patients, those with congestive heart failure, hypertensives of African origin. The higher prevalence of women in this study, mean age of the population and race, are factors that favour the use of diuretics in achieving BP control in the study population. A sore point in the study was the conspicuous absence of the use of non-pharmacological treatment option, such as body weight and lifestyle modifications. This has been documented to be associated with substantial savings in cost22 , especially in an economy as obtainable in the country. There was no documentation of body mass index (BMI), except body weight in a few subjects. Previous reports have demonstrated a higher prevalence of increased BMI in treated23 and untreated24 hypertensives in Nigeria. Advice on lifestyle modifications was documented in only 1% of the subjects. These are inconsistent with the guidelines. CONCLUSION In conclusion, hypertensives are likely to present late in this community and when they do, they commonly require multitherapy for BP control. Physicians in this hospital complied fairly with the stated guidelines. However, they do not appear to recommend lifestyle modification to their patients in the management of hypertension. REFERENCES
© Pharmacotherapy Group, Faculty of Pharmacy, University of Benin, Benin City, Nigeria. The following images related to this document are available:Photo images[pr08012t3.jpg] [pr08012t2.jpg] [pr08012t4.jpg] [pr08012f1.jpg] [pr08012t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}