 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Tropical Journal of Pharmaceutical Research, Vol. 7, No. 3, September, 2008, pp. 1025-1031 Research Article Diversity of Urinary Tract Pathogens and Drug Resistant Isolates of Escherichia Coli in different age and gender Groups of Pakistanis MF Bashir1*, JI Qazi2, N Ahmad2, and S Riaz3 1The School of Biological Sciences, Code Number: pr08023 Abstract Purpose: This paper was mainly aimed to investigate drug resistance of the various urinary tract
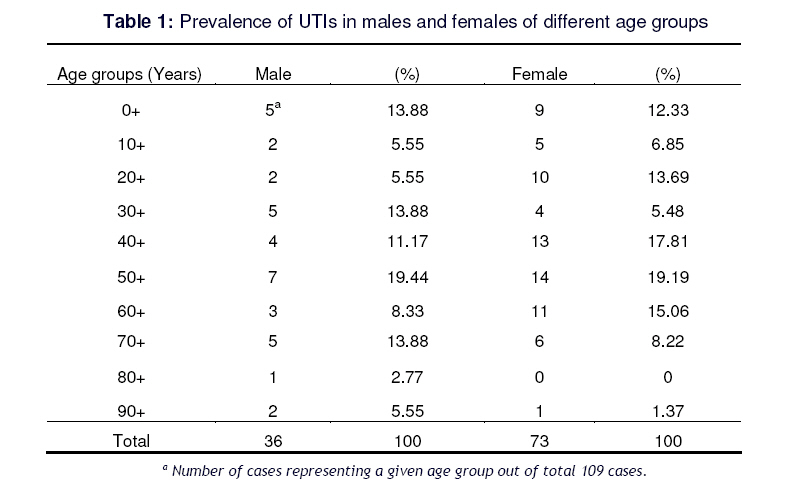
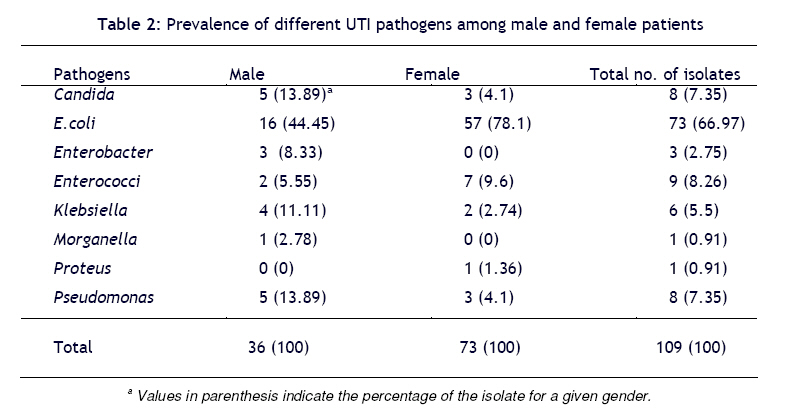
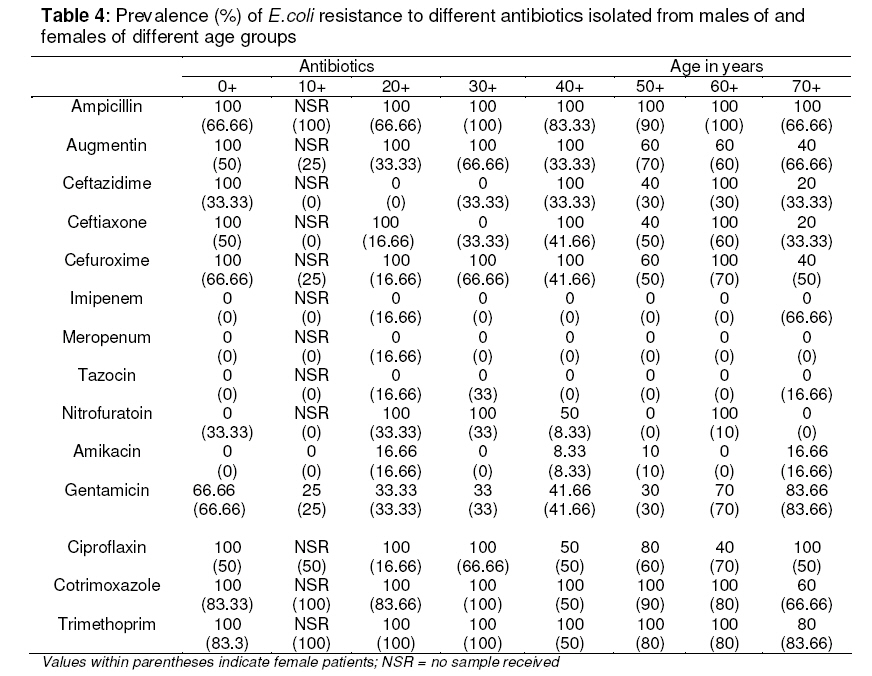
infection (UTI) pathogens from patients of different gender and age groups of Pakistanis. Keywords: Urinary tract infections, Age, Gender, Resistant microbes, E.coli. INTRODUCTION With the constantly shifting trends in drug resistance, antibiotic options, and pharmacoeconomic considerations, urinary tract infections (UTIs) continue to be one of the most frequently diagnosed cases, having an estimated figure of 150 million per annum worldwide. In fact, UTIs are the leading cause of gram-negative bacteremia in patients of all ages and are associated with a high risk of morbidity and mortality, especially in the elderly, and account for significant health care costs.1, 2 Warren et al 3 have reported that in the United States, urinary tract infections result in approximately 8 million physician visits per year. In spite of the availability and use of the antimicrobial drugs, UTIs caused by bacteria have been showing increasing trends in recent years. Much of the increase has been related to emerging antibiotic resistance in urinary tract pathogens4 . The common uropathogens identified in adult patients with UTIs include enteric gram-negative bacteria, with E. coli being the most common. The remainders of infections are caused by coagulase-negative Staphylococcus saprophyticus (10-20%), while Proteus mirabilis, Klebsiella, and Enterococcus account for less than 5%1,5,6 . Other aerobic gram-negative bacteria of the Enterobacteriacea family include Citrobacter, Enterobacter, Serratia, and Salmonella3,7. The high incidence of UTIs in the general population, the potential for complications, especially in high-risk subgroups and the associated costs of treatments emphasize the importance of appropriate antibiotic therapy. Microbial resistance to nearly all classes of antimicrobials continues to rise despite increasing awareness and concerns worldwide4,8,9,10-12 The situation is more adverse where indiscriminate use of antibiotics is rampant. In Pakistan, general practitioners, at large, recommend antibiotics without isolation and sensitivity test for pathogens. Poverty and illiteracy further strengthen the indiscriminate use of antibiotics including the low/high dose intake, incomplete course and a general trend of using left over drugs. Such practices may result an increase in resistant pathogens. The present report describes some data in this regard. For this purpose one hundred and nine positive urine samples received at Shaukat Khanum cancer hospital, Lahore were employed to isolate and characterize the pathogens for UTIs and to make comparison of antibiotics sensitivity/ resistance patterns. These data provide baseline information for further study and are useful for managing UTI cases. METHOD Study Design This study focuses on the antibiotic susceptibility patterns and frequency of uropathogens in different gender and age groups. 109 positive human urine samples obtained from different collection points and hospitalized patients at Shaukat Khanum cancer hospital and research center, Lahore were used for this purpose. These samples were processed to monitor urinary tract infection and antibiotics sensitivity patterns of pathogenic bacteria. The data were categorized viz gender and age. This study was approved from the University of the Punjab. Lahore. Study Protocols The specimens were collected for about three months between February 2004 to April 2004.The specimens which grew positive were selected for further analysis. The specimens which grew more then one type of colonies were excluded from this study. The specimens whose age or sex record were not available were also rejected. A bacterial colony count of 10,000 cfu/ml and 100,000 cfu/ml of urine for patients 0-16 years and above 16 years respectively, was selected as criterion for inclusive in the study. It is identical to that used to diagnose UTI in a number of previous studies4,8. Lactobacilli and coagulase-negative Staphylococci were considered as contaminants and were also excluded from the study. The urine samples were inoculated on cysteine lactose electrolyte deficient agar (CLED). All Gram negative rods and enterococci were identified by using conventional biochemicals plus API 20E (Biomeurex) and Oxoid Streptococcal grouping kits, respectively. Antibiotic sensitivity testing of all isolates was performed on muller hinton agar plates by Kerby-Baure disk diffusion technique with guidelines established by National Committee for Clinical Laboratory Standards ( NCCLS )13 Oral antibiotics for which uropathogens were tested include; ampicillin, trimethoprime, ciprofloxin, nitrofuratoin, augmentin, and cotrimoxazole.Parental antibiotics include; gentamicin, amikacin, imipenem, meropenem, , ceftazidime, ceftriaxone, cefuroxime, and Tazocin. Data Analysis Data were categorized viz age and sex. The patients were divided into age groups as 0+ (0-9 years), 10+ (10-19 years), 20+ (20-29 years), 30+ (30-39 years), 40+ (40-49 years), 50+ (50-59 years), 60+ (60-69 years), 70+ (70-79 years), 80+ (80-89 years) and 90+ (9099 years). RESULTS When the data were classified into different age and gender groups, it appeared that the cases of urinary tract infections (UTIs) were more in boys than girls of less than ten years of age. For the age group 20+ the females showed more than double the % of UTIs cases in males. For the next age group (30+) the situation appeared inverse to the preceding age group. Then for the age groups 40+ and 60+ females had 6.64% and 6.73% higher prevalence of the infection respectively than the corresponding male groups. However for age group 50+ gender wise difference was not prominent. For 70+ age group the cases for males appeared double than the females (Table 1). Among the uropathogens E.coli was the most frequent in both sexes with 44.45 % and 78.1% frequencies in male and female patients, respectively. Enterococci caused two folds (9.6 %) UTIs in females than the males (5.55%). Candida, Pseudomonas and Klebsiella were isolated from 13.89 %, 13.89 % and 11.11 % of the males, respectively. For females the corresponding figures were 4.1 %, 4.1% and 2.74%, respectively. The uropathogens, nterobacter (8.33 %) and Morganella (2.78 %) appeared only in males. UTI cases caused by Proteus appeared 1.36 % in females only (Table 2). When sensitivity to different antibiotics was compared, imipenen, meropenum and tazocin were found effective against the bacterial isolates from both sexes. It is surprising that all the antibiotics, except amikacin, showed more resistance in male patients than females. Nitrofuratoin showed about two folds resistance in males than females, while Trimethoprim, cotrimoxazole and ceftazidime showed 11% more resistance in males than females. Ceftriaxone, ciprofloxin, ampicillin and augmentin showed 13%, 14%, 16% and 20 % more resistance in males as compared to females, respectively (Table 3). E.coli did not show resistance to imipenen, meropenum and tazocin in all age groups of males. On the other hand the bacteria manifested almost complete resistance to ampicillin, trimethoprim and cotrimoxazole in all the age groups. The isolates from below 40 years male patients and age groups 50+ and 70+ showed almost complete resistance to ciprofloxin, while it was effective in half of male patients in age groups 40+ and 60 +. Amikacin experienced little resistance in age groups 20+(16.66 %), 40+(8.33%), 50+(10%) and 70+(16.66%), while for other age groups it was completely effective. Different trends in resistance for the different age groups are shown in this study. Bacterial isolates from females showed relatively less resistance than males. Imipenem, tazocin, meropenum and amikacin were found effective in most of the age groups, while these drugs showed 16.66% resistance in age group 20+. Nitrofurantoin showed 33% resistance in age groups 0+, 20+ and 30+ and was found almost sensitive in all other age` groups. Ampicillin faced almost complete resistance in all age groups except 0+, 20, + and 70+ for which 67% resistance was recorded. Augmentin showed variation in resistance from 25% to 70% in different age groups and was found to be sensitive in age groups 10+ and 20+. Ceftriaxone showed 60% resistance in age group 60+. ceftriaxone was sensitive in age group 10+, while it showed variable resistance among other age groups. Ciproflaxin, cotrimoxazole and trimethoprim showed variable resistance patterns in all age groups except 40+ in which these antibiotics were effective among half the female patients. (see Table 4). In general, E.coli isolates in this study showed varying patterns of antimicrobial resistance to different antibiotics viz ampicillin about (92%), trimethoprim (86%) cotrimoxazole (80%), ciprofloxin (62%), gentamicin, (49%) nitrofuratoin (20%) and amikacin (4%). Enterococci, the only gram positive isolate, was found to be susceptible to ampicillin, imipenem, penicillin, tazocin and vancomycin. The Enterococci isolates showed resistance to ceftriaxone (77.77%) and cefuroxime (66.66%). DISCUSSION The most frequent causative agent of UTIs in this study was found to be E.Coli (66.97%) followed by Enterococci (8.26%), Candida spp. and Pseodomonas spp.(7.34% each),Klebsiella spp.(5.50%), Enterobacter spp. (2.75%),Proteus spp. and Morgenella spp.(0.91% each). In two other studies in Pakistan, Khan6 reported a uropathogens prevalence of 45.6% for E. coli. This was followed by Candida spp. (10.5%), Enterococcus spp. (10.2%) while Farooqy14 revealed a prevalence of 42% for E. coli, 16% Pseudomonas aeruginosa, 11% Klebsiella aerogenes, 5.0% ,Enterobacter spp., 13% Proteus spp., 4.0% Serratia liquifaciens, 1.0%,Acinetobacter spp., 3.0% Citrobacter spp., 4.0% Enterococci and 0.5% Staphylococcus aureus. Prevalence of different pathogens is dependent on several population attributes, sample size and hygienic conditions of the patients. Therefore, a stable pattern in this regard cannot be predicted. This is why data vary when different studies are compared. For example, Hsueh et alhave reported that the most frequent isolates from UTIs at a university hospital in Taiwan during the period 1993 -1998 were Candida spp. (23.6%), E.Col i(18.6%) and P.aeruginosa (11.0%). However, in 1999, E.Coli (18.4%) replaced Candida spp. (14.3%) as the top ranking pathogen causing UTIs. The consistently high prevalence of resistance to cotrimoxazole and an increasing pattern of resistance to ciprofloxacin require ongoing surveillance to identify further changes among urinary tract isolates of E. coli16 .The in vitro activities of nitrofuratoin and the other antibiotics with even lesser resistance found in the present study suggest that they would provide adequate alternative therapy in locations where the uropathogens E.coli had developed multi drugs resistance17 Planning to reduce resistance is very important, as organisms resistant to one antimicrobial agent are likely to become resistant to others. Researchers have found that bacteria isolated from UTIs have resistance to common drugs such as ampicillin and sulphonamides in over one-third of cases. These drugs have been on the market for several decades16. In the present study when the data were visualized in different age groups for both genders, it appeared that in the case of males, E.coli isolates were susceptible to nitrofuratoin in age groups 0+, 50+ and 70+, while in age groups 20+, 30+ and 60+ hundred percent resistance was recorded. E.Coli In females, showed no resistance to nitrofuratoin in age groups 10+, 50+ and 70+, while it showed 33% resistance in age groups 0+, 20+ and 30+. E.Coli isolates from age groups 50+ and 70+ both in males and females were found to be 100% susceptible to the nitrofuration.(Table 4) Such varying pattern of resistance also appeared in different age and gender groups to other antibiotics in this study. These findings are difficult to explain. McLoughlin and Joseph18 have indicated that prevalence of resistant organisms vary by geography, patient age, and hospitalization status. The present analysis indicates the more likelihood of selective development of resistance to some antibiotics in certain age groups may have link(s) with physiological differences amongst the groups. However, such data appear beneficial to physician for empirical prescriptions of different antibiotics taking into account many age groups. The activity of the antibiotics investigated in this study against E.coli in female patients are as follows, in decreasing order: imipenem = meropenum > tazocin > amikacin > nitrofurantoin > ceftazidime > ceftriaxone >gentamicin = augmentin > cefuroxime > ampicillin. For isolates from male patients, as ciprofloxin > cotrimoxazole = trimethoprim> the order is: imipenem = meropenum = tazocin= amikacin > nitrofuratoin > ceftazidime > gentamicin > ceftriaxone > augmentin = Cefuroxime= ciprofloxin > cotrimoxazole > trimethoprim > ampicillin. Similar orders can be worked out for isolates with respect to different age groups. These resistance and susceptibility patterns should be considered in order to improve empirical antibiotic therapy in UTI cases. CONCLUSION The organisms showed resistance to older urinary antimicrobial agents such as ampicillin and cotrimoxazole; this indicates that increased consumption of a particular antibiotic can be a pathway to its resistance. Higher prevalence of UTIs was observed in female population. The prevalence of UTIs was highest for age group 50+ followed by 0+ in both genders. E.coli showed no resistance to nitrofuratoin in age groups 50+ and 70 + for both genders. ACKNOWLEDGMENT The authors wish to thank the staff of the Microbiology and Molecular Biology section, Department of Pathology, Shaukat Khanum Memorial Cancer Hospital, Lahore, Pakistan, for their assistance in the experimental work. REFERENCES
© Pharmacotherapy Group, Faculty of Pharmacy, University of Benin, Benin City, 300001 Nigeria. The following images related to this document are available:Photo images[pr08023t3.jpg] [pr08023t4.jpg] [pr08023t2.jpg] [pr08023t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}