 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Tropical Journal of Pharmaceutical Research, Vol. 8, No. 2, June 2009, pp. 161-172 Review Article Orally Disintegrating Tablets: A Review Jaysukh J Hirani1*, Dhaval A Rathod1, Kantilal R Vadalia2 1 Smt. R.D.Gardi B. Pharmacy College, Rajkot-360110, Shri H.N. Received: 30 June 2008 Revised accepted: 02 November 2008 Code Number: pr09022 Abstract Drug delivery systems are becoming increasingly sophisticated as pharmaceutical scientists acquire a better understanding of the physicochemical and biochemical parameters pertinent to their performance. Over the past three decades, orally disintegrating tablets (ODTs) have gained considerable attention as a preferred alternative to conventional tablets and capsules due to better patient compliance. ODTs are solid dosage forms containing medicinal substances which disintegrate rapidly, usually in a matter of seconds, when placed on the tongue. Products of ODT technologies entered the market in the 1980s, have grown steadily in demand, and their product pipelines are rapidly expanding. New ODT technologies address many pharmaceutical and patient needs, ranging from enhanced life-cycle management to convenient dosing for paediatric, geriatric, and psychiatric patients with dysphagia. This has encouraged both academia and industry to generate new orally disintegrating formulations and technological approaches in this field. The aim of this article is to review the development of ODTs, challenges in formulation, new ODT technologies and evaluation methodologies, suitability of drug candidates, and future prospects. Keywords: Orally disintegrating tablet, Improved bioavailability, Texture analyser, NanomeltTM Introduction For the past one decade, there has been an enhanced demand for more patient-friendly and compliant dosage forms. As a result, the demand for developing new technologies has been increasing annually1. Since the development cost of a new drug molecule is very high, efforts are now being made by pharmaceutical companies to focus on the development of new drug dosage forms for existing drugs with improved safety and efficacy together with reduced dosing frequency, and the production of more costeffective dosage forms. For most therapeutic agents used to produce systemic effects, the oral route still represents the preferred way of administration, owing to its several advantages and high patient compliance compared to many other routes2. Tablets and hard gelatin capsules constitute a major portion of drug delivery systems that are currently available. However, many patient groups such as the elderly, children, and patients who are mentally retarded, uncooperative, nauseated, or on reduced liquid-intake/diets have difficulties swallowing these dosage forms. Those who are traveling or have little access to water are similarly affected3-5 . To fulfill these medical needs, pharmaceutical technologists have developed a novel oral dosage form known as Orally Disintegrating Tablets (ODTs) which disintegrate rapidly in saliva, usually in a matter of seconds, without the need to take it water. Drug dissolution and absorption as well as onset of clinical effect and drug bioavailability may be significantly greater than those observed from conventional dosage forms6-8 . Although chewable tablets have been on the market for some time, they are not the same as the new ODTs. Patients for whom chewing is difficult or painful can use these new tablets easily. ODTs can be used easily in children who have lost their primary teeth but do not have full use of their permanent teeth9. Recent market studies indicate that more than half of the patient population prefers ODTs to other dosage forms10 and most consumers would ask their doctors for ODTs (70%), purchase ODTs (70%), or prefer ODTs to regular tablets or liquids (>80%)11 . The US Food and Drug Administration Center for Drug Evaluation and Research (CDER) defines, in the ‘Orange Book’, an ODT as “a solid dosage form containing medicinal substances, which disintegrates rapidly, usually within a matter of seconds, when placed upon the tongue”12 . The significance of these dosage forms is highlighted by the adoption of the term, “Orodispersible Tablet”, by the European Pharmacopoeia which describes it as a tablet that can be placed in oral cavity where it disperses rapidly before swallowing13 . ODT products have been developed for numerous indications ranging from migraines (for which rapid onset of action is important) to mental illness (for which patient compliance is important for treating chronic indications such as depression and schizophrenia)14 . Descriptions of Orally Disintegrating Dosage Forms ODTs are distinguished from conventional sublingual tablets, buccal tablets, and lozenges, which require more than a minute to dissolve in oral cavity. In the literature, ODTs also are called orodisperse, mouth-dissolving, quick-dissolve, fast-melt, and freeze-dried wafers. A freeze-dried wafer is a quick-dissolving, thin matrix that contains a medicinal agent that does not need water for swallowing. This fragile dosage form requires unit-dose packaging to ensure physical stability. The wafer disintegrates instantaneously in the oral cavity and releases drug, which dissolves or disperses in the saliva. The saliva is swallowed and the drug is absorbed across the gastrointestinal tract (GIT)15 . -An orally disintegrating tablet (ODT) is a solid dosage form that contains medicinal substances and disintegrates rapidly (within seconds) without water when placed on the tongue. The drug is released, dissolved, or dispersed in the saliva, and then swallowed and absorbed across the GIT13 . A quick-dissolving tablet (also known as a fast-dissolving, fast-dissolving multiparticulate, rapid-dissolving, mouth-dissolving, fastmelting, or orodispersing tablets) is an oral tablet that does not require water for swallowing. The tablet dissolves within 60 seconds when placed in the mouth. The active ingredients are absorbed through mucous membranes in the mouth and GIT and enter the blood stream. A fraction of pregastric drug absorption may bypass the digestive system and metabolism by the stomach acids and enzymes. In general, the tablets are physically robust and can be packaged in multidose containers16 . Ideal properties of ODTs The performance of ODTs depends on the technology used during their manufacture. The necessary property of such tablets is the ability to disintegrate rapidly and disperse or dissolve in saliva, thereby obviating the need for water. Various technologies have been developed that enable ODT to perform this unique function. An ideal ODT should meet the following criteria:
The Need for Development of ODTS The need for non-invasive delivery systems persists due to patients’ poor acceptance of, and compliance with, existing delivery regimes, limited market size for drug companies and drug uses, coupled with high cost of disease management. Patient factors17-20 Orally disintegrating dosage forms are particularly suitable for patients, who for one reason or the other, find it inconvenient to swallow traditional tablets and capsules with an 8-oz glass of water. These include the following:
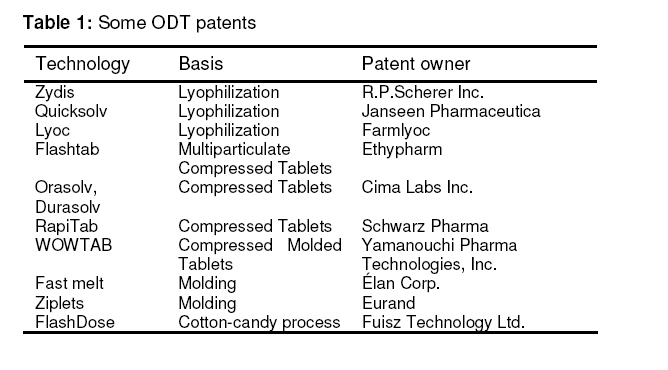
Effectiveness factor Increased bioavailability and faster onset of action are a major claim of these formulations. Dispersion in saliva in oral cavity causes pregastric absorption from some formulations in those cases where drug dissolves quickly. Buccal, pharyngeal and gastric regions are all areas of absorption for many drugs21 . Any pregastric absorption avoids first pass metabolism and can be a great advantage in drugs that undergo a great deal of hepatic metabolism. Furthermore, safety profiles may be improved for drugs that produce significant amounts of toxic metabolites mediated by first-pass liver metabolism and gastric metabolism, and for drugs that have substantial fraction of absorption in the oral cavity and pregastric segments of GIT22 . Manufacturing and marketing factors Developing new drug delivery technologies and utilizing them in product development is critical for pharmaceutical industries to survive, regardless of their size. As a drug nears the end of its patent life, it is common for pharmaceutical manufacturers to develop a given drug entity in a new and improved dosage form. A new dosage form allows manufacturer to extend market exclusivity, unique product differentiation, value-added product line extension, and extend patent protection, while offering its patient population a more convenient dosage form. This leads to increased revenue, while also targeting underserved and under-treated patient populations23 . As examples, Eisai Inc. launched Aricept ODT, a line extension of donepezil for Alzheimer’s disease, in Japan in 2004 and in the U.S. in 2005 in response to a generic challenge filed in the U.S. by Ranbaxy. Merck’s Japanese subsidiary launched Lipola M (simvastatin ODT), a line extension of its block-buster, Zocor®, a cholesterol-lowering drug, in response to seventeen generic registrations of simvastatin applied for in Japan in 200424 . Marketers build a better brand and company image when they offer a unique easier-to-take form that satisfies the need of an underserved patient population. Challenges in Formulating ODTS Palatability11,25 As most drugs are unpalatable, orally disintegrating drug delivery systems usually contain the medicament in a taste-masked form. Delivery systems disintegrate or dissolve in patient’s oral cavity, thus releasing the active ingredients which come in contact with the taste buds; hence, taste-masking of the drugs becomes critical to patient compliance. Mechanical strength19,26,27 In order to allow ODTs to disintegrate in the oral cavity, they are made of either very porous and soft-molded matrices or compressed into tablets with very low compression force, which makes the tablets friable and/or brittle, difficult to handle, and often requiring specialized peel-off blister packing that may add to the cost. Only few technologies can produce tablets that are sufficiently hard and durable to allow them to be packaged in multidose bottles, such as Wowtab® by Yamanouchi-Shaklee, and Durasolv® by CIMA labs. Hygroscopicity28 Several orally disintegrating dosage forms are hygroscopic and cannot maintain physical integrity under normal conditions of temperature and humidity. Hence, they need protection from humidity which calls for specialized product packaging. Amount of drug11,14 The application of technologies used for ODTs is limited by the amount of drug that can be incorporated into each unit dose. For lyophilized dosage forms, the drug dose must be lower than 400 mg for insoluble drugs and less than 60 mg for soluble drugs. This parameter is particularly challenging when formulating a fast-dissolving oral films or wafers. Aqueous solubility7,29 Water-soluble drugs pose various formulation challenges because they form eutectic mixtures, which result in freezing-point depression and the formation of a glassy solid that may collapse upon drying because of loss of supporting structure during the sublimation process. Such collapse sometimes can be prevented by using various matrix-forming excipients such as mannitol than can induce crystallinity and hence, impart rigidity to the amorphous composite. Size of tablet30 The degree of ease when taking a tablet depends on its size. It has been reported that the easiest size of tablet to swallow is 7-8 mm while the easiest size to handle was one larger than 8 mm. Therefore, the tablet size that is both easy to take and easy to handle is difficult to achieve. Selection of ODT Drug Candidates Several factors must be considered when selecting drug candidates for delivery as ODT dosage forms. In general, an ODT is formulated as a bioequivalent line extension of an existing oral dosage form. Under this circumstance, it is assumed that the absorption of a drug molecule from the ODT occurs in the postgastric GIT segments, similar to the conventional oral dosage form. But this scenario may not always be the case. An ODT may have varying degrees of pregastric absorption and thus, the pharmacokinetic profiles will vary.29 Therefore, the ODT will not be bioequivalent to the conventional oral dosage form. For example, ODT formulations of selegiline, apomorphine, and buspirone have significantly different pharmacokinetic profiles compared with the same dose administered in a conventional dosage form31,32 . It is possible that these differences may, in part, be attributed to the drug molecule, formulation, or a combination of both. If significantly higher plasma levels have been observed, pregastric absorption leading to the avoidance of first-pass metabolism may play an important role. This situation may have implications for drug safety and efficacy, which may need to be addressed and assessed in a marketing application for an ODT33 . For example, safety profiles may be improved for drugs that produce a significant amount of toxic metabolites mediated by firstpass liver metabolism and gastric metabolism and for drugs that have a substantial fraction of absorption in the oral cavity and segments of the pregastric GIT. Drugs having ability to diffuse and partition into the epithelium of the upper GIT (log P > 1, or preferable > 2); and those able to permeate oral mucosal tissue are considered ideal for ODT formulations. Patients who concurrently take anticholinergic medications may not be the best candidates for these drugs. Similarly, patients with Sjögren’s syndrome or dryness of the mouth due to decreased saliva production may not be good candidates for these tablet formulations20 . Drugs with a short half-life and frequent dosing, drugs which are very bitter or otherwise unacceptable taste because taste masking cannot be achieved or those which require controlled or sustained release are unsuitable candidates of rapidly dissolving oral dosage forms. Researchers have formulated ODT for various categories of drugs used for therapy in which rapid peak plasma concentration is required to achieve the desired pharmacological response. These include neuroleptics, cardiovascular agents, analgesics, antiallergic, anti-epileptics, anxiolytics, sedatives, hypnotics, diuretics, anti-parkinsonism agents, anti-bacterial agents and drugs used for erectile dysfunction34 . Approaches to ODT Development The fast disintegrating property of the tablet is attributable to a quick ingress of water into the tablet matrix resulting in its rapid disintegration. Hence, the basic approaches to develop rapidly dissolving oral dosage forms include maximizing the porous structure of the tablet matrix, incorporating the appropriate disintegrating agent and using highly watersoluble excipients in the formulation35 . As is often the case, a technology that is originally developed to address a particular administration need can quickly become adopted as part of a pharmaceutical company’s product life cycle management strategy, which is precisely what has happened with ODT technologies. Several patented technologies with their basis of formulation are listed in Table 1. The technologies that have been used by various researchers to prepare orally disintegrating dosage forms include: Freeze-Drying or Lyophilization, Molding, Direct Compression, Disintegrant addition, Sublimation, Spray Drying, Mass Extrusion, Cotton-candy process, NanoCrystalTM Technology, Oral films/wafers. Specific properties of the various ODT technologies are listed in Table 2. Broadening the scope of ODT technologies Industry observers point to broadening uses of ODT technology. These include the incorporation of macromolecules using ODT into vaccines. The success for other peptide and protein products will depend on Another emerging area is the wider application of ‘oral thin-strip technologies’. The use of thin-film strips is of growing interest in the pharmaceutical sector following the success of Listerine PocketPaks® in the United States. Thin-film strip technology uses a range of water-soluble polymers and is reported to be able to incorporate watersoluble, insoluble, or taste-masked ingredients. The film is manufactured as a continuous sheet and then cut into individual doses prior to packing. The major limitations to this technology are the relatively low doses that can be accommodated (approximately 30 mg) and its moisture sensitivity thus requiring specific unit-dose packaging to protect the product and ensure shelf life. Thin-film technology has primarily been used in overthe-counter (OTC) products36 (see Table 3). Companies with oral thin-film technologies and products include LTS Lohmann Therapy Systems (West Caldwell, NI), Adhesives Research (Glen Rock, PA), Applied Pharma Research (Balerna, Switzerland), and Meldex International (Cambridge, UK)37 . Elan’s proprietary NanoCrystal technology (NanomeltTM)38 can enable formulation as well as improve compound activity and final product characteristics. Decreasing particle size increases the surface area, which leads to an increase in dissolution rate. This can be accomplished predictably and efficiently using NanoCrystal technology. NanoCrystal particles are small particles of drug substance, typically less than 1000 nm in diameter, which are produced by milling the drug substance using a proprietary wet milling technique. This technology provides for pharmacokinetic benefits of orally administered nanoparticles (less than 2 microns) in the form of a rapidly disintegrating tablet matrix and wide range of doses (up to 200mg of API per unit). NanoCrystal colloidal dispersions of drug substance are combined with water-soluble GRAS (generally regarded as safe) ingredients, filled into blisters, and lyophilized. The resultant wafers are remarkably robust, yet dissolve in very small quantities of water in seconds. This approach is especially attractive when working with highly potent or hazardous materials because it avoids manufacturing operations (granulation, blending, and tableting) that generate large quantities of aerosolized powder and present much higher risk of exposure. ODT Evaluation of Special Concern Crushing strength and friability can be assessed as stated in pharmacopoeias. But some tests are of special concern and these include the following: Wetting time Wetting time of dosage form is related to the contact angle. It needs to be assessed to give an insight into the disintegration properties of the tablets; a lower wetting time implies a quicker disintegration of the tablet. For this purpose, a tablet is placed on a piece of tissue paper folded twice and kept in a small Petri dish (ID = 6.5 cm) containing 6 ml of water, and the time for complete wetting is measured39 . Disintegration test The time for disintegration of ODTs is generally less than one minute and actual disintegration time that patient can experience ranges from 5-30 seconds. The standard procedure of performing disintegration test for these dosage forms has several limitations and they are not suitable for the measurement of very short disintegration times. The method needs to be modified for ODTs as disintegration is required without water; thus the test should mimic disintegration in salivary contents. A modified dissolution apparatus is applied to an ODT with a disintegration time that is too fast to distinguish differences between tablets when the compendial method is used. A basket sinker containing the tablets is placed just below the water surface in a container with 900 mL of water at 37 0C, and a paddle rotating at 100 rpm is used. The disintegration time is determined when the tablet has completely disintegrated and passed through the screen of the sinker40 . Various scientists41 have developed new in vitro methods that allow an accurate determination of disintegration test. The disintegration test is performed using a texture analyzer instrument. In this test, a flat-ended cylindrical probe penetrates into the disintegrating tablet immersed in water. As the tablet disintegrates, the instrument is set to maintain a small force for a determined period of time. The plots of some distance traveled by the probe generated with the instrument’s software provide disintegration profile of the tablets as a function of time. The plot facilitates calculation of the start and end-point of the tablet disintegration. Dissolution test42 The development of dissolution methods for ODTs is comparable to the approach taken for conventional tablets, and is practically identical. Dissolution conditions for drugs listed in a pharmacopoeia monograph, is a good place to start with scouting runs for a bioequivalent ODT. Other media such as 0.1 M HCl and buffer (pH 4.5 and 6.8) should be evaluated for ODT much in the same way as their ordinary tablet counterparts. It has been suggested that USP 2 paddle apparatus is the most suitable and common choice for orally disintegrating tablets, with a paddle speed of 50 rpm commonly used. Moisture uptake studies43 Moisture uptake studies for ODT should be conducted to have an insight into the stability of the formulation, as several excipients used are hygroscopic. Ten tablets from each formulation are kept in a desiccator over calcium chloride at 370C for 24 h. The tablets are then weighed and exposed to 75% RH at room temperature for two weeks. The required humidity (75% RH) is achieved by keeping saturated sodium chloride solution at the bottom of the desiccator for three days. One tablet as control (without superdisintegrant) is kept to assess the moisture uptake due to other excipients. Tablets are weighed and the percentage increase in weight is recorded. Clinical studies In vivo studies have been performed on oral fast-disintegrating dosage forms to investigate their behavior in the oral–esophageal tract, their pharmacokinetic and therapeutic efficacy, and acceptability. Zydis’s residence time in the mouth and stomach, and its transit through the esophageal tract, was investigated using gamma-scintigraphy. Its dissolution and buccal clearance was rapid44 ; the esophageal transit time and stomach emptying time were comparable with those of traditional tablets, capsules, or liquid forms. A decreased intersubject variability in transit time was also observed45,46 . Zydis also showed good therapeutic efficacy and patient acceptability -particularly in children47,48 or when easy administration and rapid onset of action were required (such as for patients undergoing surgery)49,50 . The fastdisintegrating forms examined showed improved pharmacokinetic characteristics when compared with reference oral solid formulations. For example, the absorption rate of the acetaminophen Flashtab was higher than that of the brand leader, while having the same bioavailability51 . Increased bioavailability and improved patient compliance were observed in Lyoc formulations for different drugs such as phloroglucinol52 , glafenine52 , spironolactone53 , and propyphenazone54 . Using Zydis, all the drugs that can be absorbed through the buccal and esophageal mucosa exhibited increased bioavailability and side-effect reduction. This is helpful particularly in actives with marked first-pass hepatic metabolism44 . Finally, the suitability of ODTs for long-term therapy was also assessed. Lyoc formulations containing aluminum were positively tested in patients with gastrointestinal symptoms55 . Counseling points for ODTs20 Pharmacists are in the ideal position to become familiar with the various technologies, and educate their patients on what to expect upon taking their first dose. The majority of patients receiving ODT formulations have little understanding of this new dosage form. Patients may be surprised when tablets begin to dissolve in the oral cavity. They might expect a faster onset of therapeutic action. Clarification from the pharmacist can avoid any confusion or misunderstanding. Although no water is needed to allow the drug to disperse quickly and efficiently, most technologies utilize the body’s own salivation. Decreased volume of saliva may slow the rate of disintegration/dissolution and decrease the bioavailability of the product. Although chewable tablets have been in the market for some time, they are not the same as the new ODTs. Patients for whom chewing is difficult or painful can use these new tablets easily. ODTs can be used easily in children who have lost their primary teeth, but do not have full use of their permanent teeth. Patients may mistake ODTs for effervescent tablets. Pharmacists may wish to stress the difference between the use of ODTs and effervescent tablets. ODT formulations are more susceptible to degradation via temperature and humidity. Some of the newest ODT formulations are dispensed in a conventional stock bottle. Pharmacists are advised to take care when dispensing such formulations to ensure they are not exposed to high levels of moisture or humidity. As with most drugs, patients should be advised to avoid storing ODTs in the medicine cabinet in the bathroom. Pharmacists have been alerted to exercise additional care when dispensing new prescriptions for ODT formulations. Most such products are available in the same strengths as traditional dosage forms. Prescribing physicians must make an additional notation for the dispensing of an ODT. A physician may also mistakenly believe the drug brand name is Zydis, for example, without identifying a specific drug. Verification with the prescribing practitioner may be necessary in some cases and can clear up any confusion. Industrial Applications Industrial applications include the following:
Future Prospects These dosage forms may be suitable for the oral delivery of drugs such as protein and peptide-based therapeutics that have limited bioavailability when administered by conventional tablets. These products usually degrade rapidly in the stomach. Should next generation drugs be predominantly protein or peptide based, tablets may no longer be the dominant format for dosing such moieties. Injections generally are not favored for use by patients unless facilitated by sophisticated auto-injectors. Inhalation is one good alternative system to deliver these drugs, but the increased research into biopharmaceuticals so far has generated predominantly chemical entities with low molecular weights. The developments of enhanced oral protein delivery technology by ODTs which may release these drugs in the oral cavity are very promising for the delivery of high molecular weight protein and peptide. Conclusion Orally disintegrating tablets have better patient acceptance and compliance and may offer improved biopharmaceutical properties, improved efficacy, and better safety compared with conventional oral dosage forms. Prescription ODT products initially were developed to overcome the difficulty in swallowing conventional tablets among pediatric, geriatric, and psychiatric patients with dysphagia. Today, ODTs are more widely available as OTC products for the treatment of allergies, cold, and flu symptoms. The target population has expanded to those who want convenient dosing anywhere, anytime, without water. The potential for such dosage forms is promising because of the availability of new technologies combined with strong market acceptance and patient demand. By paying close attention to advances in technologies, pharmaceutical companies can take advantage of ODTs for product line extensions or for first-to-market products. With continued development of new pharmaceutical excipients, one can expect the emergence of more novel technologies for ODTs in the days to come. References
© Pharmacotherapy Group, Faculty of Pharmacy, University of Benin, Benin City, 300001 Nigeria. The following images related to this document are available:Photo images[pr09022t2.jpg] [pr09022t1.jpg] [pr09022t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}