 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Tropical Journal of Pharmaceutical Research, Vol. 8, No. 4, Aug, 2009, pp.303-310 Research Article Clinical Features, Complications and Treatment Outcome of Brucella infection: Ten Years' Experience in an Endemic Area HA Bukharie Department of Internal
Medicine, Division of Infectious Disease, King Fahd Hospital of the University,
Alkhobar, Saudi Arabia Received: 13 January 2009 Code Number: pr09039 Abstract Purpose: Brucellosis is a multi-systemic
infection that is endemic in some parts of the world. The purpose of this study
was to examine the epidemiology as well as the clinical and haematological
characteristics, complications, and treatment outcome of patients with
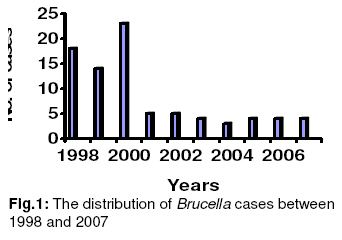
brucellosis at the King Fahd Hospital of the University Alkhobar, Saudi Arabia. Key words: Brucellosis; Recurrent fever; Saudi Arabia; Ascites; Arthritis; Menstrual cycle. INTRODUCTION Brucellosis is a disease of domestic and wild animals that can be transmitted to humans (zoonosis). The disease exists worldwide, particularly in the Mediterranean basin, the Arabian Peninsula, the Indian subcontinent, and in parts of Mexico and Central and South America1. Consumption of contaminated foods and occupational contact remain the main sources of infection1. Human brucellosismay present with protean clinicalmanifestations that require broad differential diagnosis, includingmany infectious and noninfectiousdiseases. It isa systemic infection that can affect any organ inthe body¹. The onset of disease is insidious in approximately half of all cases. It is characterized by several somatic complaints such as fever, sweats, anorexia, and weight loss. By contrast, there can be few abnormal physical findings. Occasionally, symptoms related to a single organ predominate. The aim of this study was to examine the epidemiological features, clinical and haematological characteristics, complications, and treatment outcomes of brucellosis in an endemic region. PATIENTS AND METHODS Study population Between 1998 and 2007, a descriptive case assessment of 84 adult patients with brucellosis presented to King Fahd Hospital of the University, Alkhobar, in a longitudinal prospective study. The university hospital is a secondary–tertiary care hospital in the Eastern Province of Saudi Arabia. Diagnostic criteria The diagnosis of brucellosis was based on the clinical findings characteristic of the disease and on either positive cultures that tested for Brucella species or a titre of ≥ 1: 160 antibodies by tube agglutination. Complete blood count, sedimentation rate, liver function tests, and in some patients detection of immunoglobulin (IgM and IgG) antibodies by ELISA were also performed. Treatment and outcome Various treatment combinations of anti-Brucella antimicrobials (streptomycin, doxycycline, co-trimoxazole, rifampicin, ciprofloxacin) were used, depending on the patient’s age and pregnancy status. The mean follow-up period was one year, although this was not possible for all patients because of the nomadic nature of the patient population. Relapse was defined as an initial improvement followed by reappearance of symptoms and signs during the treatment period or within 2 months of discontinuation of treatment. A cure was defined as no recurrence of symptoms and signs during the 12-month follow-up period. RESULTS A total of 84 patients were diagnosed with brucellosis during the 10-year study. The number of patients with brucellosis reduced during the study period, with a much smaller number of cases occurring after 2000 (Fig. 1). The median age of patients was 32±9 years (range: 13–81 years). Males were more often affected than females and the male-to-female ratio was 3:1. Of the 84 patients, two presented with a relapse, while the other 82 were diagnosed with brucellosis for the first time. Fifty four patients (64%) gave history of contact with animals, sixteen patients (19%) gave history of drinking raw milk, five patients (6%) were involved in slaughtering animals particularly during Hajj season, three patients (4%) were laboratory workers, and six patients (7%) denied any risk factors for acquiring brucellosis. The occupations of the patients varied from farmers (21 males and 2 females), Sheppard (12 males, and 1 female), students (8 males and 4 females), teachers (6 males and 3 female), laboratory workers (2 males, and 1 female), engineer (I male), housemaid (1 female), housewives (18 females), and unemployed (4 males). The clinical characteristics of the 84 patients with brucellosis are described in Table 1. A history of fever was obtained from 95% of patients, but it was positive in 73% of patients. A substantial number of patients (64%) developed arthritis or arthralgia. Splenomegaly was recorded in 13 (16%) and hepatomegaly in 9 (11%) patients. Two patients presented with fever of unknown origin with negative serology and only bone marrow culture was positive for Brucella mellitensis. Two patients presented with recurrent fever associated with menstruation. Table 1: Clinical characteristics and laboratory findings of 84 patients with brucellosis
SAT – standard tubeagglutination test, ALT – alanine aminotransferase, AST – aspartate aminotransferase One previously healthy patient presented with jaundice and spontaneous peritonitis. The diagnosis was confirmed after isolating Brucella melitensis from blood and by complete resolution of symptoms with treatment. Eleven patients (13%) presented with generalized lymphadenopathy. Seven patients (8%) had epididymo-orchitis. Neurological and cardiac involvement was infrequent. One patient had meningitis and another patient presented with endocarditis. Laboratory data Erythrocyte sedimentation rate (ESR) was measured in all patients and it ranged from 4 to 110 mm/hour (median 35 mm/hour). Thirty patients (36%) had anaemia(haemoglobin concentration <11.5 g/dLin females and <13.5g/dL in males). Five patients had leukocytosis (>10,500 white blood cells [WBCs]/mm3), and five patients had leukopaenia (<4500WBCs/mm3). Lymphocytosis was seen in 50 patients (60%). Three patients (4%) had thrombocytopenia (<150,000platelets/mm3). Twenty-four (29%) patients had slight-to-moderately increased serum hepatic transaminaselevels. Thirty-one patients (37%) had increasedserum g-glutamyl transpeptidase (GGT)and alkaline phosphatase concentrationswith normal bilirubin levels(dissociated cholestasis). Standardtube agglutination testing ofinitial samples from 80(95%) of the 84patients was positive forantibodies to Brucella (titre,³ 1: 160). Cultures of specimensfrom 33 (39%) of the 84 patientswere positive for Brucellaspecies, thirty-one were isolated from blood samples, and two from bone marrow aspirates. Only 18 of the 33 Brucella isolates were speciated; this was because some isolates died, some specimens were discarded, or laboratory reagents were not available. Of these 18 isolates, twelve (67%) were B. melitensis and six (33%) were Brucella abortus. Antimicrobial susceptibility testing was carried out on 33 isolates. The number of Brucella isolates with antimicrobial resistance was as follows: 12 (36%) were resistant to co-trimoxazole; 6 (18%) were resistant to rifampicin; all isolates were susceptible to tetracycline, streptomycin, and ciprofloxacin. ELISA wasperformed to test for IgM and IgG antibodies in 28 patients, and only 18 (64%) were positive for IgM or IgG antibodies. A positive result was noted in 8 of 23 patients (34%) for culture-confirmed brucellosis. Treatment and rate of relapse Treatment regimens for the 84 patients consisted of combinations of two or three agents: streptomycin plus doxycycline (18%); doxycycline plus rifampicin (18%); doxycycline plus co-trimoxazole (12%); rifampicin plus co-trimoxazole (2%); doxycycline plus ciprofloxacin (31%); and streptomycin plus doxycycline plus ciprofloxacin (19%). Streptomycin was administered for 15 days. Treatment with other antimicrobial agents varied according to clinical response and the development of complications (mainly arthritis). Spondylitis is recognized as the most common and one of the most debilitating forms of focal brucellosis and there is no consensus on the best therapeutic regimens, so we chose triple therapy (doxycycline, streptomycin, and ciprofloxacin) to treat patients with Brucella spondylitis. A total of 61 patients (73%) had long-term follow-up (12 months). Six patients (7%) suffered a relapse after completion of therapy with no osteoarticular or nervous system involvement. Three of these six patients had received doxycycline and co-trimoxazole. Isolates from two patients were found to be resistant to co-trimoxazole and the isolate from the third patient failed to grow. Three patients relapsed after receiving doxycycline and rifampicin. Blood cultures of both of these patients tested negative for Brucella. None of the patients who received streptomycin or ciprofloxacin in combination with doxycycline suffered a relapse (Table 2). Table 2: Treatment and outcome for 84 patients with brucellosis
Note: The proportion ofpatients (%) receiving each regimen are shown; Dox – doxycycline; Rif – rifampin; Stm – streptomycin; TMP-SMZ – trimethoprim-sulfamethoxazole; cipro – ciprofloxacin DISCUSSION Brucella is one of the world's main zoonotic pathogens, and is responsible for enormous economic losses, as well as considerable human morbidity in endemic areas.Brucellosis has been present for thousands of years and has managedto elude eradication2 even in the most developed countries2-4, .It is well known to have ahigh prevalence in certain geographic areas, such as the Mediterranean basin, the Arabian Peninsula, the Indian subcontinent, and South America1-4. Transmission of brucellosisto humans occurs through the consumptionof infected, unpasteurized animal-milk products, by directcontact with infected animal parts (such as the placenta byinoculation through ruptures of skin and mucous membranes),and through the inhalation of infected aerosolized particles. Brucellosis is an occupational disease for shepherds, abattoirworkers, veterinarians, dairy-industry professionals, and personnelin microbiologic laboratories. The number of patients with brucellosis in our hospital reduced over the 10-year study period, with a much smaller proportion of cases occurring after 2000. This is due to the concerted efforts of public health measures such as public education, milk pasteurization, and livestock immunization. In addition, increased awareness of the disease among physicians, improved laboratory diagnosis, and treatment of cases by primary care physicians may also have contributed to this reduction5. Human brucellosis is traditionally described as a disease ofprotean manifestations, and the demographicand clinical characteristics ofthe patients in thisstudy emphasize the wide and unexpected spectrum of this disease. The characteristics of fever vary and canbe spiking and accompanied by rigors,or may be relapsing, mild, or protracted. Constitutional symptoms are generallypresent. Dissemination via the bloodstream can result in involvement of almost any organ and the clinical presentation can be misleading and cases in which gastrointestinal, respiratory, dermal, or neurological manifestations predominate are not uncommon6-10. However neurological or cardiovascular manifestation were rare in our patients . The results of physical examinations are often nonspecific, althoughlymphadenopathy, hepatomegaly, or splenomegaly is often present. Hepatomegaly was observed in 9% of cases, whereas splenomegaly and lymphadenopathy were present in 13% of cases. Osteoarticular disease is the most common complicationof brucellosis, and was reported in 64% of patients in our study. There are three distinct forms: peripheralarthritis, sacroilitis, and spondylitis. The reproductive system is the second most common site of focalbrucellosis. Brucellosis can present as epididymo-orchitis inmen and is often difficult to differentiate from other localdisease11. Brucellosisduring pregnancy is associated with a substantial risk of spontaneous abortion12. We diagnosed epididymo-orchitis in seven patients, and one patient had an abortion. Hepatitis is common, usually manifesting as mild transaminasemia13,14. In our study 29% of patients had increased enzyme concentrations (ALT, AST). Jaundice is usually rare and only one of the patients in our study presented with jaundice, together with spontaneous peritonitis. The patient had no underlying condition such as chronic liver disease, congestive heart failure, nor was she on peritoneal dialysis. Brucellosis is a rare cause of bacterial peritonitis. Few cases have been reported, and most were associated with chronic liver disease15. The other patients had underlying conditions such as ascites caused by congestive heart failure15and in patients undergoing CAPD16. Our patient had complete resolution of symptoms with treatment. Two patients presented with menstrual associated recurrent fever. Although brucellosis is known to cause recurrent fever, the association with menstrual cycle to my knowledge has never been reported. Abnormal bloodtest results are usuallymild and nonspecific. Changes in blood count are often due to mild leukopaenia andrelative lymphocytosis, together with mild anaemia and thrombocytopaenia. The most common haematological manifestations in our study were anaemia, lymphocytosis, and moderate increases in the sedimentation rate. In our study, one patient presented with pancytopenia. Pancytopaenia in brucellosis is multifactorial and has been attributedto hypersplenism and bone marrow involvement. The absolute diagnosis of brucellosis requires isolation ofthe bacterium from blood or tissue samples, or the combination of clinical symptoms and positive serology. The sensitivityof blood culture varies, depending on individual laboratory practices and how the cultures are obtained. Positive blood cultures are found in 15to 70% of patients with brucellosis17. In our study, positive cultures were obtained from 37% of blood and 2% of bone marrow samples of patients with brucellosis. Prior use of antibiotics is associated with reduced incidence of positive blood cultures but does not affect bone marrow culture. In two cases, patients had positive bone marrow cultures despite all other negative diagnostic tests for Brucella. A bone marrow culture is recommended for patients with fever of unknown origin, negative serology, and unexplained joint or hematological involvement in whom brucellosis is suspected18. The presumptivediagnosis of brucellosiscan be made serologically in conjunction with compatibleclinical presentation19. Positive results (titersof antibodies to Brucellaof ³ 1: 160 [standard tubeagglutination test] or ³ 1: 320 [Coombs' test]) are common, although low titers, determined by standard tubeagglutination tests, have beenreported18. In rarecases patients with brucellosis can have positive bloodcultures but negative serology20. Two of the patients in our study with Brucella bacteremia had negative serology on repeated occasions. More recently, the Brucella enzyme-linked immunosorbent assay (ELISA) test has been introduced into clinical laboratories for the diagnosis of brucellosis. The ELISA test is reported to be rapid, highly sensitive, and specific for detecting the Brucella-specific IgG, IgM, and IgA antibodies in blood and cerebrospinal fluid21. In our study, in patients with Brucella bacteremia the sensitivity of the ELISA IgM or IgG tests were lower than the sensitivity of the standard tube agglutination tests; this finding has also been reported by others22. The successful treatment of brucellosis requires prolonged chemotherapy regimen with a combination of antibiotics. In 1986, the World Health Organization issued guidelines forthe treatment of human brucellosis23. The guidelines recommend tworegimens, both involved doxycycline for six weeks andin combination with either streptomycin for two to three weeksor rifampin for six weeks. Both combination regimens are the most populartreatments worldwide, although they are not used universally.The streptomycin-containing regimen is slightly more effective in preventing relapse24. However,parenteral administration of streptomycin requires either hospitaladmission or an adequate health care network— both of which are often absent from areas of endemic disease.On the other hand, the use of rifampin in areas in which brucellosisis endemic, and where tuberculosis is also usually endemic, raisesconcerns about the development of community resistance to rifampin. Al –Hajjaj et al documented worsening resistance in the Riyadh Region between 1986 and 1997 for both rifampicin and streptomycin25. The likely culprits are poor compliance and the wide use of rifampin and streptomycin for the treatment of brucellosis and other conditions. Alternative drug combinations have been used, including otheraminoglycosides (e.g., gentamicin and netilmicin), trimethoprim–sulfamethoxazolecombination and quinolones. A recent meta-analysis of the efficacy of various combinationsto treat spondylitis advocated treatment for at leastthree months; however, the superiority of one specific regimen couldnot be proved24, but preliminary results indicate that quinolones may be cost-effective in spondylitis26. In this study, patients received various chemotherapy regimens. The duration of therapy was based on the level of organ involvement. No therapeutic failure was observed with any of the regimens, but the relapse rate was 7%. None of the patients who received streptomycin or ciprofloxacin in combination with doxycycline had a relapse. A regimen of doxycycline and ciprofloxacin is significantly more expensive than the traditional regimens. However, when the protracted duration of other treatment regimens, the economic impact of the residual damage and the economic consequences are considered, the combination of doxycycline and ciprofloxacin may prove cost-effective. CONCLUSION The clinical presentations among our patients emphasize the wide and unexpected spectrum of this disease. Timely diagnosis and treatment of patients with brucellosis require clinical awareness of the full spectrum of signs and symptoms associated with brucellosis, as delay in treatment can result in significant morbidity. REFERENCES
© Pharmacotherapy Group, Faculty of Pharmacy, University of Benin, Benin City, 300001 Nigeria. The following images related to this document are available:Photo images[pr09039f1.jpg] |
| |||||||||

{kind=link}