 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Tropical Journal of Pharmaceutical Research, Vol. 8, No. 4, Aug, 2009, pp. 311-316 Research Article In-vivo Kinetics of Silymarin (Milk Thistle) on Healthy Male Volunteers Muhammad Usman*, Mahmood Ahmad, Asad Ullah Madni, Naveed Akhtar, Waheed Asghar, Muhammad Akhtar, M Atif and M Qamar-uz-zaman Department of
Pharmacy, the Islamia University of Bahawalpur, Punjab, Pakistan. Received: 24 January 2009 Code Number: pr09040 Abstract Purpose:
The study was aimed at evaluating the in vivo kinetics of silymarin tablets, a
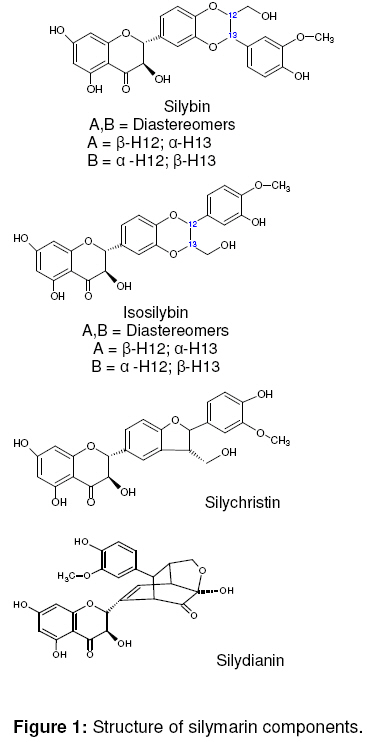
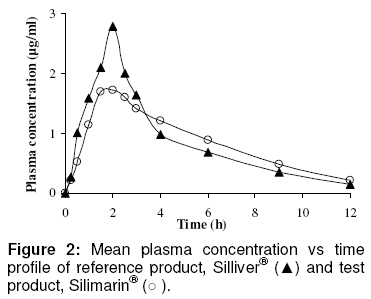
product with anti-hepatotoxic and free radical scavenging activities. Keywords: In vivo kinetics, Silymarin, Milk thistle, RP-HPLC, Pharmacokinetics. INTRODUCTION Silymarin is an active extract of the seeds of Silybum marianum (milk thistle)1. A standardized extract of the seed contains approximately 70-80% of silymarin flavonolignans and 20-30% chemically undefined fraction, comprising mostly polymeric and oxidized polyphenolic compounds2. The main component of silymarin (Figure 1) is silybin or silibinin which is a mixture of diastereomers, namely, silybin A and silybin B. Isosilybin, dehydrosilybin, silychristin, silydianin are present in considerable amounts and a few flavonoids, such as taxifolin, are also present but in small amounts2. It is reported in literature that silymarin does not possess high bioavailability3-8. Silymarin absorption rate levels are between 20 and 50%6. In fact, this poor bioavailability could be attributed to degradation by gastric fluid6, poor enteral absorption5,8 or its poor water solubility3,4,6,7. Silymarin (an extract from Silybum marianum) contains silybin as a main component and, therefore, pharmacokinetic and bioavailability studies are always based on the determination of silybin in plasma9-11. Complex composition and the ever-increasing list of their putative active constituents in an herbal extract make bioavailability and pharmacokinetic studies problematic and task becomes even more difficult when the active constituents and synergistic interactions are not fully known12. Silymarin is one of the few herbal drugs whose active constituents have been sufficiently studied and on which bioavailability studies are possible13. Therefore, this work was designed and conducted to provide pharmacokinetic data on silymarin tablets that would facilitate the rational usage of this valuable medicinal agent, which is widely used in a variety of situations, especially in liver diseases. EXPERIMENTAL Subjects and Methods Healthy male volunteers ranging in age from 22-40 years (23.1 ± 0.4 years), in weight from 55-70 kg (62.5 ± 1.3 kg), and in height from 165-180 cm (176.0 ± 1.8 cm) were enrolled according to the inclusion/exclusion criteria of Food and Drug Administration (FDA)14. Pharmacy Ethical Committee of the Faculty of Pharmacy and Alternative Medicine, the Islamia University of Bahawalpur, approved the study protocols for the human studies. Written informed consent was obtained from each volunteer who received an oral dose (200mg) of silymarin of both products according to a randomized cross-over design. A washout period of one week was allowed between the two treatments. The subjects were housed at the study centre throughout period of blood sampling. Approximately 3 ml aliquot of blood sample was collected pre-dose (to serve as a control), and over a period of 12 h after sylimarin administration. The blood was centrifuged immediately and plasma was stored at -70 0C until HPLC analysis. HPLC analysis Preparation of the mobile phase The mobile phase consisted of methanol and potassium dihydrogen phosphate buffer (20 mM) in a ratio of 50:50 v/v with the pH of the buffer adjusted to 2.8 with phosphoric acid. It was filtered through a 0.45µm membrane filter before use. The flow rate was 1 ml/min at 30 0C. Detection was performed at 288 nm15. Preparation of stock solutions A stock solution of silymarin was prepared fresh by dissolving 50 mg drug in 50 ml of methanol to give a final concentration of 1 mg/ml. Working solutions of silymarin were prepared in the mobile phase by appropriate dilution (2.5, 15, 30, 62.5, 125, 250 and 500 µg/ml). All the solutions were stored at -20 0C, protected from light. Preparation of standard curve A standard curve was constructed to encompass anticipated range of plasma silymarin concentration found in healthy volunteers. The curve was prepared by spiking different samples of 1ml plasma each with 20 µl of one of the working solutions to produce calibration curve points equivalent to 0.05, 0.3, 0.6, 1.25, 2.5, 5.0 and 10 µg/ml of silymarin. Aliquots of 100 µl were injected and spectra were taken in each case and the peak areas noted. The intra-day (within-run) and inter-day (between-run) accuracy and precision of the method were determined on three separate days. Extraction procedure An aliquot (100 µl) of acetate buffer (pH 5.6) and a 30 µl aliquot of β-glucuronidase Type HP-2 (Helix pomatia-Merck, Germany, 1,27300 units/ml) were added to a 100µl aliquot of plasma sample and the mixtures were incubated at 37 C˚ for 2 h with periodical shaking. Then 200µl of borate buffer (pH 8.5) and 2.0 ml of diethyl ether were added to the mixture. The mixture was vortexed for 1 min and centrifuged at 3000 rpm for 2 min. The organic phase was transferred into a clean sample test tube and evaporated under a gentle stream of nitrogen. The residue was reconstituted in a 130 µl aliquot of the mobile phase, vortexed for 30 seconds and centrifuged for 1 min at 2500 rpm, and then 100 µl of the solution was injected directly into the chromatographic system15. Pharmacokinetic analysis Pharmacokinetic parameters were calculated using the pharmacokinetic software, Kinetica version 4.4 and MS Excel 2007. The rate and extent of absorption was measured by Cmax, Tmax and AUC0-∞ for both the reference and test products. Maximum concentration of silymarin in plasma (Cmax), time to reach peak plasma concentrations (Tmax) and area under the curve (AUC0-∞) were calculated by the trapezoidal rule. All other parameters - plasma half life (t1/2), elimination rate constant (Ke), volume of distribution (Vd), total body clearance (ClT) and mean residence time (MRT) - weredetermined with the aid of the software. Statistical analysis of data Paired t-test was applied for the determination of statistical difference between the values of the bioavailability and pharmacokinetic parameters of the two brands of silymarin using Med. Calculator and MS-Excel software at the 95% confidence level. RESULTS The results of (mean ± SEM) plasma concentration versus time profiles for all the volunteers that received the treatments are plotted in Figure 2. Table 1 represents the values of bioavailability and other pharmacokinetic parameters. The values of AUC0-∞ for the two products (10.8 ± 0.4 and 11.2 ± 0.7 µg h/ml for the test and reference, respectively) were not significantly different (P < 0.05). The maximum plasma concentration (Cmax) of the reference and test products were 2.9 ± 0.3 and 1.9 ± 0.1 µg/ml, respectively, and the difference was significant (p < 0.05). However, the Tmax of the reference and test products, which were 1.9 ± 0.1 and 1.8 ± 0.1 h, respectively, are not significantly different (P > 0.05). Other pharmacokinetic parameters evaluated did not show any statistical difference (P < 0.05) between the two products except mean residence time which was significantly different. They are (for reference and test products, respectively): elimination rate constant (Ke) - 0.3 ± 0.01 and 0.2 ± 0.02 h-1 (in a previous study, Ke was reported as 0.3 ± 0.08 h-1 16); mean residence time (MRT) - 4.6 ± 0.2 and 6.1 ± 0.4 h; plasma half life (t1/2) - 2.8 ± 0.1 and 3.536 ± 0.403 h; volume of distribution (Vd) - 1.2 ± 0.1 and 1.5 ± 0.2 L/Kg; total body clearance (ClT) - 303.5 ± 44.1and 297.4 ± 62.6 ml h-1 Kg-1 Table 1: Comparative bioavailability and pharmacokinetic parameters of Silliver®-Abbott and Silimarin®-Amson administered in an oral dose of 200 mg to normal male subjects (mean ± SEM).
* = pharmacokinetic parameter; s = Signifiant difference (P<0.05); ns = non signifiant difference (P>0.05) DISCUSSION The task of in vivo evaluation of herbal medicines is difficult due to complex composition, ever-increasing list of their putative active constituents and specific analytical method12,13. Woo et al17 reported the value of AUC0-∞ as 22.75 ± 3.19 µg h/ml after the administration of silymarin capsule to rats at a dose of 140 mg/Kg. The difference between reported17 and present AUC values is due to differences in dose, dosage form, and experimental subjects. Therefore, it is evident that AUC0-∞ values in the present study a similar trend as in the previous studies. The variation in the values of Cmax of the two brands may be due to differences in the nature and source of the raw materials for the silymarin. It has been well documented that the proportion of active constituents in various silymarins depends largely on the source of Silybum marianum seeds. Moreover, various other factors - environmental, cultivation, drying and processing procedures - can also influence the concentration of active ingredients. Silymarin is also extracted from the fruits of Silybum marianum instead of the seeds17. Silymarin extracted from the fruits of Silybum marianum may contain varied concentration of active principles which can lead to variation in Cmax. Another probable reason for the difference in Cmax values may be differences in the extraction procedures for the sylimarins used in the manufacture of the two products. Differences in formulation and processing variables could also have influenced the release of the drugs from the drug products, resulting in dissimilar Cmax values. The value of the bioavailability coefficient (F), calculated as 0.96 at 90% confidence interval, and the area under the curve (AUC) ratio should generally be within the acceptance range of 80-125%. CONCLUSION On the basis of the F (bioavailability coefficient) values and the AUC which fell in the range 80-125%, it can be said that Silimarin®-Amson can be used as a substitute for the better known brand, Silliver®-Abbott in healthy human subjects except in situations where the maximum plasma concentrations of the latter must be attained , e.g., in acute conditions such as acute pain. However, the test product should be suitable for use in chronic conditions such as hepatitis. ACKNOWLEDGEMENT The authors are thankful to Amson Vaccines & Pharma (Pvt.) Ltd, Islamabad, Pakistan for their support for this study REFERENCES
© Pharmacotherapy Group, Faculty of Pharmacy, University of Benin, Benin City, 300001 Nigeria. The following images related to this document are available:Photo images[pr09040f1.jpg] [pr09040f2.jpg] |
| |||||||||

{kind=link}
{kind=link}