 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Tropical Journal of Pharmaceutical Research, Vol. 9, No. 5, September-October, 2010, pp. 431-439 Research Article Angiotensin Converting Enzyme Insertion/Deletion Gene Polymorphism: An Observational Study among Diabetic Hypertensive Subjects in Malaysia Jaime Jacqueline Jayapalan1 , Sekaran Muniandy1* and Chan Siew Pheng2 1Department of Molecular Medicine, 2Department of Medicine, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia *Corresponding author: Email: sekaran@um.edu.my; Tel: +603-7967 4953; Fax: +603-7967 4957 Received: 27 October 2009 Revised accepted: 3 July 2010 Code Number: pr10051 Abstract Purpose: This study investigated the influence of angiotensin-1 converting enzyme (ACE) insertiondeletion
(ID) gene polymorphism on the treatment responses of type 2 diabetic subjects at varying
stages of nephropathy to ACE inhibitors (ACEI) with regard to blood pressure (MAP) and renal response
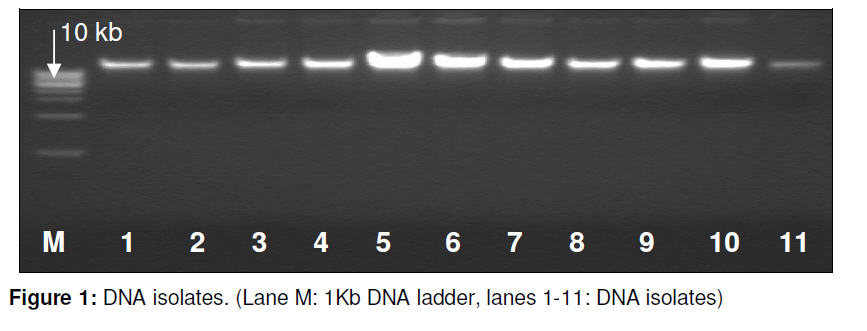
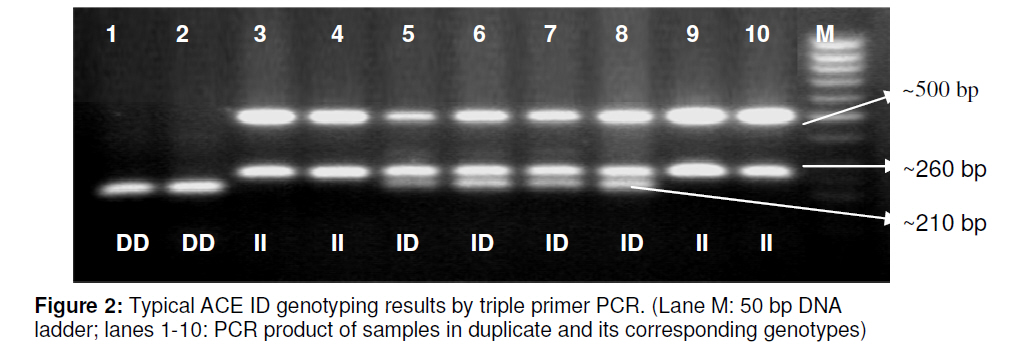
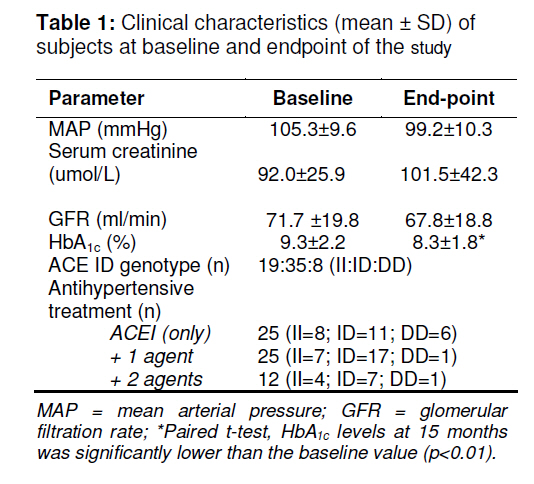
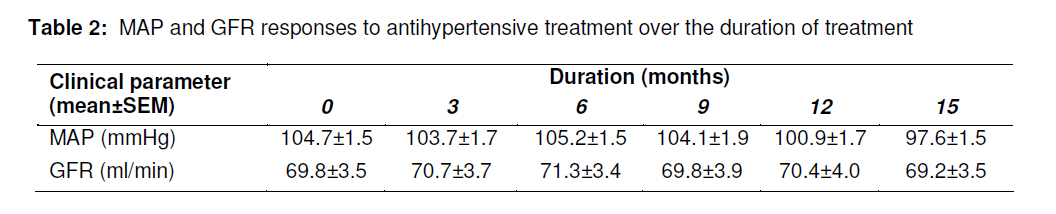
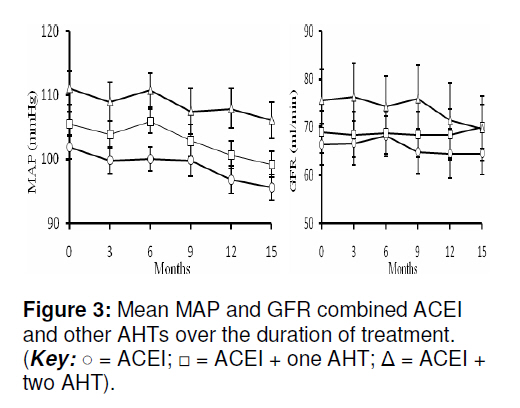
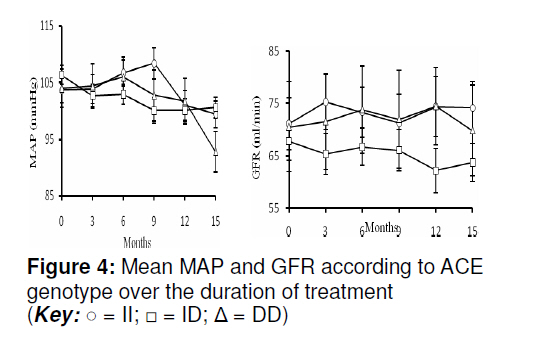
(GFR). Keywords: ACE genotype, ACE inhibitor, Type 2 diabetes mellitus, Diabetic nephropathy INTRODUCTION Many trial-proven strategies have been developed in preventing and delaying the progression of nephropathy in patients with diabetes. Maintenance of tight blood glucose and blood pressure controls, encouraging weight reduction and cessation of smoking, treating dyslipidaemia, restricting intake of protein diet, prescribing acute high or chronic low doses of erythropoietin and early identification and referral of patients with potential risk for developing end-stage renal failure are some of the diabetic nephropathy management strategies being practiced in primary health care settings for subjects at risk for developing diabetic nephropathy [1-2]. In addition, novel therapies including sulodexide, a glycosaminoglycan, pyridoxamine, an advanced glycation end product inhibitor, ruboxistaurin, a protein kinase C inhibitor and aliskiren, a renin inhibitor are promising in retarding disease progression of diabetic nephropathy both in animal models and small clinical studies [3]. Antihypertensive treatment (AHT), particularly the use of ACE inhibitors (ACEI), have been reported to show beneficial reno-protective effects in patients with diabetic and nondiabetic nephropathy [4]. ACEIs execute hypotensive effects by decreasing the formation of a potent vasoconstrictor, angiotensin-II and by decreasing the degradation of the potent vasodilator, bradykinin while affecting glomerular haemodynamics by decreasing the glomerular capillary pressure. They also have an antiproteinuric effect superior to other AHTs [5]. The II, ID and DD genotypes resulting from the polymorphic site of the ACE gene have been shown to have low, intermediate and high plasma expression, respectively. With that, the II genotype has been thought to confer protective benefits while DD genotype, is believed to confer deleterious effects on various disease pathogenetic mechanism particularly, diabetic nephropathy [6]. In addition, characterization of the ACE ID gene polymorphism has also been suggested for decision making regarding antihypertensive treatment regimens [7]. Hence, we investigated the role of ACE ID gene polymorphism in Malaysian diabetic nephropathic subjects in determining the effect of ACE inhibitors on mean arterial pressure (MAP) and glomerular filtration rate (GFR) in a short-term observational retrospective study. Additionally, we have also assessed the concomitant use of additional antihypertensive drugs to ACEI on the changes of mean MAP and GFR over time in these subjects. METHODS Patient selection Enrolment of subjects was conducted at the outpatient diabetes/nephrology clinic at the University of Malaya Medical Center (UMMC), Kuala Lumpur. Approval from the Medical Ethics Committee (UMMC) and informed consent from all recruited subjects were obtained. A total of 256 patients with varying stages of nephropathy were reviewed for the study. Following a thorough review of the medical records of these subjects, only a total of 62 subjects with type 2 diabetes mellitus (T2DM) and with a mean age (±SD) of 60.5 ± 8.4 (male: 38.7 %; female: 61.2 %) were selected for this retrospective observational study. Among these, 37 subjects were also on one or two antihypertensive drugs in addition to ACEI. They had been on ACEIs consecutively for over 15 months with complete medical records from 2001 to 2007. All the diabetic patients included were hypertensive (BP> 140/90 mmHg) and with varying degrees of kidney damage (ranging from stages I – III) [8] prior to ACEI treatment. Clinical characteristics Mean arterial pressure (MAP) was approximated by the equation, {2/3 * diastolic blood pressure (DBP)} + {1/3 * systolic blood pressure (SBP)}. The ratio of total haemoglobin (Hb) to HbA1C concentration expressed by glycosylated hemoglobin (HbA1c) concentration in percentage, determined by cyanide-free colorimetric and latex agglutination method, respectively, was computed [9]. The glomerular filtration rate (GFR) was estimated by Cockcroft-Gault (CG) equation [10] as in Eq 1. GFR ml/min = {(140 - age) x weight (kg)} / {72 x serum creatinine (mg/dl)} ……………….……... (1). ACE ID genotyping Highly purified and concentrated genomic deoxyribonucleic acid (DNA) was isolated using the WizardR Genomic DNA purification kit (Promega, Madison) based on a series of lysis, precipitation and desalting procedures. The DNA was then subjected to triple primer polymerase chain reaction (PCR) amplification of the insertion/deletion (I/D) polymorphic site of the ACE gene as previously described [11]. Briefly, PCR was performed in a final volume of 25μl containing 10mM Tris-HCl (pH 8.8), 50mM KCl, 0.8% Nonidet P40, 1.5mM MgCl2, 0.2mM dNTPs, 20pmol of each primer (Forward: 5’-CCC ATC CTT TCT CCC ATT TCT C-3’, Nested: 5’-GGT TTC ACC GTT TTA GCC GGG A-3’ and Reverse: 5’-CCA TGC CCA TAA CAG GTC TTC A-3’ primers, 1U Taq DNA Polymerase (Fermentas, Lithuania), and ~100ng of genomic DNA. The optimized PCR run includes an initial denaturation at 94 oC for 3 min, followed by 30 cycles of denaturation at 94 oC for 30 s, annealing at 64 oC for 30 s, and extension at 72 oC for 30 s, and a final extension at 72 oC for 7 min in an Eppendorf Master Thermal Cycler (Eppendorf, Hamburg). Subsequently, following agarose gel (1.5 %) electrophoresis, ACE I/D genotyping was determined based on the discriminating band size pattern where band sizes of approximately 500 bp and 260 bp designated the II genotype, while band sizes of approximately 500 bp, 260 bp and 210 bp designated the ID genotype and a single band with a size of approximately 210 bp indicates the DD genotype. ACE inhibitors (ACEI) observational retrospective study For the retrospective study, blood pressure readings were recorded from the subject’s respective medical records at 3 monthly intervals. Subsequently, the MAP was estimated thus, showing a total of 6 readings for the period under study. C-G equationsbased GFR measures were estimated as well. Zero (0) month is the onset point of drug administration, and therefore, considered as the baseline value. Statistical analysis Statistical Package for Social Sciences version 14.0 (Chicago, Illinois) was used to perform statistical analysis. Paired samples Students t-test was used to compare the means of HbA1c level between baseline and at month 15. Parametric one-way ANOVA procedure was used to test the mean MAP and GFR differences between the subgroups: (a) ACE genotype subgroups – II : ID : DD, and (b) Pharmacologic therapy subgroup– ACEI : ACEI + one AHT : ACEI + two AHT , at baseline. Post-hoc analysis was carried out using the Tukey post-hoc test as equal variances were assumed. The general linear model (GLM) repeated measures were applied to study the effects of ACE inhibitors on MAP and GFR over the period. Mauchly’s sphericity test was used to assess the assumption of sphericity, while the Bonferonni procedure was used to perform pairwise comparison between the groups of means. A p value of < 0.05 was considered statistically significant. RESULTS ACE ID genotyping and clinical characteristics Typical gel presentation showing the isolated DNA and PCR amplicons banding pattern based ACE ID genotyping are shown in Figures 1 and 2, respectively. Clinical characteristics of the subjects at both baseline and end-point are shown in Table 1. Table 1 indicates that homozygous insertion (II) alleles were found in 19 (30.6 %) patients while heterozygous insertion-deletion (ID) alleles and homozygous deletion alleles (DD) were found in 35 (56.5 %) and 8 patients (12.9 %), respectively. In terms of the antihypertensive therapy (AHT) regimens that had been administered to these subjects, 40.3 % of the patients were on ACE inhibitors alone while 40.3% and 19.4% were on one and two additional antihypertensive agents, respectively (Table 1. The commonly used ACEI drugs include perindopril, lisinopril, enalapril and captopril, in that order. The types of drugs used in combination with ACE inhibitors were dihydropyridine calciumchannel blockers (CCBs) including amlodipine, nifedipine and felodipine, as well as diuretics - thiazide and furosemide. Responses of MAP and GFR to antihypertensive treatment The p value for Mauchly test for all parameters tested was more than 0.05, hence the assumption of sphericity was met (p > 0.05). As expected, test of within- subjects effects showed a significant difference in the changes of mean MAP (p = 0.001, Observed power, 95.6 %) but not in mean GFR (p = 0.963) over 15 months (see Table 2). Using the Bonferonni pairwise comparison, we found that there was a significant difference in mean MAP measures between months 1, 3, 6 and 15. Influence of combining other additional antihypertensive agents with ACEI on MAP and GFR Assessment of the influence of combining other AHTs with ACEI on mean MAP and GFR over time is shown in Figure 3. At baseline, the mean MAP of the subgroup on ACEI with 2 additional antihypertensive drugs was significantly higher compared to those on ACEI alone (p = 0.03; Tukey post hoc test, p< 0.05). However, the mean baseline GFR between the subgroups (p = 0.929) was not significantly different. Based on the test of between-subjects effects, it was observed that there was a significant mean MAP change between subgroups (p < 0.00; Observed power, 99 %) but not in the mean GFR (p = 0.575) over time (Figure 3). Bonferonni pairwise comparisons showed a significantly lower mean MAP at 15 months from the baseline mean MAP among those on ACE inhibitors with two additional antihypertensive agents. Impact of ACE ID gene polymorphism on MAP and GFR and antihypertensive treatment outcomes Mean MAP and GFR were similar when stratified according to ACE ID genotypes at baseline (p = 0.537 and 0.571, respectively). Further test of between-subjects effects between mean MAP and GFR and ACE ID genotypes gave p values of 0.634 and 0.372, respectively, indicating that there were no significant mean MAP and GFR changes between the subgroups over time (Figure 4). Influence of ACE ID gene polymorphism on MAP and GFR for ACEI alone Changes in the mean MAP and GFR were also evaluated in subjects who were exclusively treated with ACEI (n = 25; II = 8, ID = 11, DD = 6). And again, no significant changes in both the MAP (p > 0.05) and GFR (p > 0.05) between subgroups were observed (data not shown). DISCUSSION The aim of this retrospective study was to observe the influence of ACE ID gene polymorphism on the responses of MAP and GFR to ACE inhibitors over period of 15 months. The effects of other antihypertensive agents administered concurrently with ACEI on changes of MAP and GFR over this period were also assessed. The study revealed that (a) ACEI exerted the expected hypotensive effect and maintained renal function (GFR) among the T2DM subjects with variable baseline degrees of renal insufficiency for that duration of time, and (b) ACE ID gene polymorphism had no demonstrable influence on the antihypertensive effects or the maintenance of kidney function among these subjects. MAP Overall, the use of antihypertensive agents (ACE inhibitor alone or with other second-line agents) significantly decreased the MAP from baseline values. ACEIs had been used as first line therapy among these subjects as recommended [12]. Only in uncontrolled BP situations, second-line agents were added. In the present study, aggressive use of additional antihypertensive agents were only prescribed for patients with MAP ~110 mmHg (SBP/DBP, 150/90). In such subjects, the dihydropyridine CCBs and diuretics were the only types of drugs used as second-line antihypertensive agents. These agents are well documented for exerting hypotensive effects, especially when given in combination with ACEI [13]. Similarly in the present study, a higher magnitude of change in mean MAP was observed among those on ACEI with two additional antihypertensive agents indicating synergistic drug interaction. The observed erratic change in MAP averages among subjects between clinic visits is presumably attributable to poor compliance to treatment. Non-compliance including failure to replenish prescription, consumption of incorrect dose, irregular timing, forgetfulness, and premature discontinuation of drugs would generally prove to be significant impediments to effective treatment [14]. GFR Cockcroft-Gault equations were used to estimate GFR which, in turn, was used as a marker to assess renal function of the subjects. Alternatively, the Modified Diet in Renal Disease (MDRD) equation may also be used for this purpose [15]. Although neither serves as an adequate GFR predicting formula, cost effectiveness and test convenience renders them acceptable for short-term studies [16]. Over the 15-month duration of the study, GFR was maintained at baseline values. The natural course of diabetic nephropathy has an average decline in GFR of 10 - 15 ml/min/year [1]. Hence, AHT regimens including ACEI as monotherapy or in combination with dihydropyridine CCBs and diuretics, have served their purpose by maintaining kidney function and preventing further decline in GFR. As this is a retrospective study, it is rather difficult to determine the class of antihypertensive agents that contributed most to GFR maintenance especially when GFR trend were similar in all the subgroups compared (ACEI vs ACEI+one AHT vs ACEI+two AHTs), irrespective of the class/number of antihypertensive agents used. A critical appraisal of the data suggests that there was no significant synergistic antiproteinuric effect of dihydropyridine CCBs and diuretic type of antihypertensive drugs in the present study, unlike other studies that reported beneficial renoprotective effect when other drugs such as angiotensin II receptor antagonist [17] and potassium-sparring diuretics [18] were used in combination with ACEIs. This implies that ACEI, a common denominator in all the subgroups may have been the major contributor to GFR maintenance. Although the protective influence of ACE inhibition against deterioration in renal function is well known as it exerts both anti-hypertensive as well as anti-proteinuric effects [4,5], the GFR maintenance observed in the present study may also have been influenced by improved blood pressure and glycaemic control among the subjects, as HbA1C values at month 15 were significantly lower than at baseline. A prospective observational study had previously associated incidences of diabetes complications with glycaemic exposure. Reduction in haemoglobin A1c by 1 % correlated with a decrease in risk for microvascular complications and end-point or death related to diabetes by 37 and 21 %, respectively [19]. Therefore, further validation based on a long-term (observational) study involving additional judiciously selected subgroups (such as a non-ACEI subgroup) may be necessary to confirm this assertion. ACE ID gene polymorphism Therapeutic outcomes of ACE inhibition were previously attributed to polymorphism of the ACE gene. DD genotype is associated with high-level availability of Ang-II and lower availability level of bradykinin in the kidneys, causing higher efferent arteriolar resistance and intraglomerular pressure while patients with ID and II genotype have an intermediate and decreased level of vascular and renal activity, respectively [6]. Hence, ACE inhibition was associated with improved survival and renoprotection, with the beneficial effects more pronounced in subjects with the II and ID genotypes [7]. In contrast, Scharplatz et al [20] showed a better response to ACE inhibitors in Caucasian DD genotype carriers compared to II genotype carriers in terms of blood pressure, proteinuria, GFR, ACE activity and progression to ESRF in a preliminary systematic review. In the present study however, there was no apparent impact of ACE ID gene polymorphism on the outcomes of antihypertensive therapy with regards to MAP and GFR in the subjects with diabetic nephropathy. The influence of ACE ID gene polymorphisms on the treatment outcome with ACE inhibitors have previously been demonstrated in subjects with type 1 diabetic nephropathy [21] and type 2 diabetic nephropathy [6,7] and non-diabetic nephropathies [22]. Although our finding is in contrast to these studies, but it is in agreement with reports by van der Kleij et al [23] and Schelleman et al [24] in non-diabetic renal disease and hypertensive subjects, respectively. The authors reported that the decline in GFR and blood pressure, in the latter study, in response to ACE inhibition was not affected by ACE genotype. Limitations of this study The observed lack of association between genotype and response to ACE inhibition in the present study could be due to the variation in the pharmacokinetics and pharmacodynamics of the type of ACE inhibitors [25] prescribed for the subjects. Furthermore, the small sample size involved in the study made it impossible to assess the effects of genotype for the different ACE inhibitors separately. In addition, short duration of follow-up period [23], as well as heterogeneity in ethnicity [26] and gender [27] may also have hampered a significant association of ACE genotypes. Further studies exclusively designed to accommodate these pharmacologic and demographic factors is deemed necessary to confirm our present finding of null influence of ACE ID gene polymorphism on response to ACE inhibitors. CONCLUSION In this study on Malaysian diabetic subjects, ACE ID gene polymorphism had little impact on the efficacy of ACE inhibitor therapy with regard to MAP and GFR. ACKNOWLEDGEMENT This work was funded by UM–PPP Grant P0103/2006B and PS290/2007B. Also, the authors wish to express their deep gratitude to Assoc Prof. Dr Karuthan Chinna of UITM, Malaysia, who assisted with the statistics used in this work. REFERENCES
Copyright 2010 - Tropical Journal of Pharmaceutical Research The following images related to this document are available:Photo images[pr10051f4.jpg] [pr10051t2.jpg] [pr10051f2.jpg] [pr10051f1.jpg] [pr10051f3.jpg] [pr10051t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}