 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
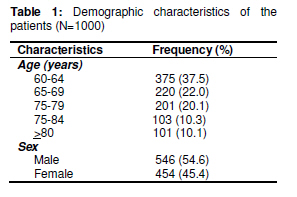
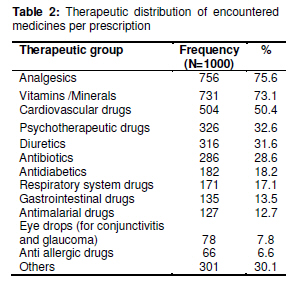
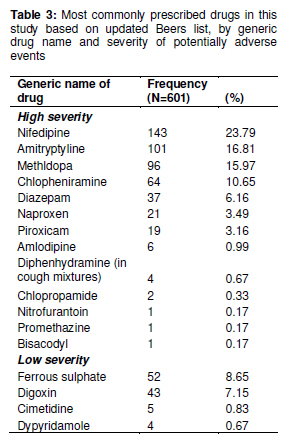
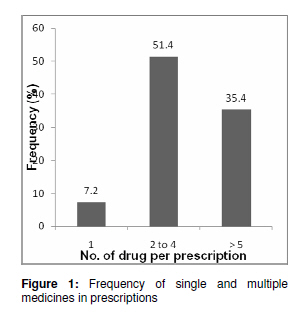
Tropical Journal of Pharmaceutical Research February 2011; 10 (1): 19-25 Research Article Prescribing Patterns and Inappropriate Use of Medications in Elderly Outpatients in a Tertiary Hospital in Nigeria Uchenna IH Eze1* and Adebiyi O Olowu2 1Department of Clinical Pharmacy and Biopharmacy, *Corresponding author: E-mail: ifyeze3000@yahoo.com; Tel: +234(0)7060627667, (0)8055481547 Received: 2 July 2010 Revised accepted: 24 January 2011 Code Number: pr11004 Abstract Purpose: To determine the prescribing patterns and occurrence of potentially inappropriate medications (PIM) among elderly outpatients visiting a tertiary hospital in Nigeria. Keywords: Elderly, Medications, Drug utilization, Potentially inappropriate medications. Introduction In spite of the widespread use of prescription drugs by the aged population, prescribing for the elderly may be less than optimal [1] and research has documented widespread inappropriate medication prescribing for the elderly [2]. Factors such as patient age, multiple diseases and disease severity, use of multiple medications, physicians’ lack of training in geriatrics as well as changes in pharmacokinetics and pharmacodynamics in elderly patients often result in increase in the incidence of drug toxicity and adverse drug reactions (ADRs) [3]. The identification of the quantity and type of prescribing problems are fundamental first steps in trying to improve the quality of prescribing and medication safety. Both require that rational drug prescribing be promoted and potentially dangerous prescribing patterns be detected quickly [4] and discouraged. Much drugrelated morbidity in the elderly population may be avoidable as it is due to inappropriate prescribing [5]. Beers et al developed criteria for identifying potentially inappropriate medications [6,7]. Their recommendations focused on drugs that should be avoided or not given, excessive dosing and excessive duration of treatment. Using Beer’s list, one-fourth of all elderly people living in a community were prescribed an inappropriate medication [8]. An updated Beers’ list stated criteria defining medications that generally should be avoided in elderly patients, regardless of the setting [9]. Studies pertaining to prescription drugs have been carried out in Nigeria [10-13]; however, there is paucity of studies combining prescribing patterns and inappropriate prescribing in a special population such as the elderly. Hence, the main aim of this study was to determine the utilization of prescription drugs and occurrence of potentially inappropriate medications among elderly outpatients attending a tertiary hospital in Sagamu, Nigeria. Specific objectives include to describe the pattern of prescription medicines (therapeutic groups) issued to elderly patients; to evaluate prescribing practices using WHO core prescribing indicators; and to ascertain the extent of potentially inappropriate prescribing for elderly patients using explicit criteria. Methods Study design A retrospective study was carried out using prescriptions (encounters) issued to elderly patients, 60 years and above, attending the outpatient clinics of Olabisi Onabanjo University Teaching Hospital (OOUTH), Sagamu, western Nigeria. This hospital is a 218-bed facility which also serves as a referral centre Sample size and selection A total of 1000 prescriptions for patients ≥ 60 years old emanating from different outpatient clinics of the hospital were consecutively selected. This large sample size, which exceeded the minimum of 100 suggested by WHO [14], was employed in order to enhance the reliability of the results since only one health facility was used in the study. Data collection A WHO prescriber indicator form [14] was used to collect and record demographic information obtained from the selected prescriptions. Other data collected include prescribing indicators such as the total number of medicines prescribed as generics and name of prescribed medicine according to therapeutic group. The extent of potentially inappropriate outpatient prescribing for these elderly patients was ascertained using Beer’s updated criteria [9]. Data analysis For easy sorting, the data obtained were entered into Microsoft Excel 2000 and Graph Pad software, version 2.05a (Graph Pad Software Inc, San Digeo, USA) was used for further analysis. P < 0.05 was interpreted as significant. The mean and standard deviation of the categorical variables stated above were obtained. Test of significance was carried out using z score and p value of ≤ >0.05 was taken to be significant. Analysis for inappropriate prescribing was based on Beer’s updated list of medications that generally should be avoided in elderly patients independent of diagnosis [9]. Procedure for calculating prescribing indicators Average number of drugs per encounter was calculated by dividing the total number of drugs prescribed by the number of prescriptions surveyed. Percentage of drugs prescribed by generic name was determined by dividing the number of drugs prescribed by generic name by the total number of drugs, which was then multiplied by 100. Percentage of encounters with an antibiotic and injection prescription was calculated by dividing the number of patient encounters during which an antibiotic or an injection was prescribed by the total number of encounters surveyed, which was then multiplied by 100, respectively. Percentage of drugs prescribed from the essential drug list was determined by dividing the number of products prescribed from the essential drug list of the hospital by the total number of drugs prescribed, and then multiplied by 100. Results Demographics The demographic characteristics of the patients are shown in Table 1. Out of 1000 prescriptions studied, 546 (54.6 %) belonged to women and the rest (454 or 45.4 %) to men, giving a female to male ratio of 1:0.83. The mean age was 68.9 ± 7.3years. Prescribed medicines The distribution of the medicines prescribed into their therapeutic groups is shown in Table 2. Analgesics were the most prescribed medicines (N = 756, 75.6 %) with acetylsalicylic acid (ASA) being the most prescribed analgesic (35.4 %). Vitamins and minerals (N = 731, 73.1 %) ranked second while cardiovascular drugs such as antihypertensives (nifedipine, methyldopa, lisinopril, etc), antianginal drugs (glyceryl tinitrate and iso-sorbide dinitrate) and cardiac glycosides (digoxin) made up 504 (50.4%) of presecriptions. Psychotherapeutic drugs occurred in 326 (32.6 %) of the prescriptions and the major groups encountered were hypnotics and sedatives (bromazepam, nitrazepam, etc) constituting 185 (56.7 %), tricyclic antidepressants (amitrptyline) 101 (30.9 %), anticonvulsants (carbamazepine) 34 (10.4 %) and antipsychotics (haloperidol and chlopromaxine) 6 (1.8 %). Diuretics occurred in 316 (31.6 %) of the prescriptions with amiloride + hydrochlorothiazide being the most prescribed with 129 (40.8 %). Thirty one different antibacterials were prescribed, with cotrimoxazole (N = 145, 15.7 %) being the single most prescribed antibacterial. More females received all therapeutic groups of drugs except for cardiovascular, antidiabetic and respiratory tract and antiallergy drugs. However, there was a significant difference between males and females in respect of vitamins and minerals (z = -10.71, p = < 0.001), antidiabetics (z = 4.33, p = 0.0001) and psychotherapeutic agents (z = -3.23,p = 0.0268) respectively. Only marginal significant gender difference was obtained for respiratory agents (z = 1.93, p = 0.0268). WHO prescribing indicators The distribution of the number of medicines prescribed is shown in Figure 1. Average number of medicines per encounter The average number of medicines per prescription was 3.9; the range being 1 to 11 medicines. Percentage of medicines prescribed by generic name A total of 1945 (48.9 %) of the drugs were prescribed in their generic names with 58 % of them having at least 1-2 medicines written in generics. Percentage of encounters with an antibiotic prescribed Two hundred and thirty (23 %) prescriptions had one or more antibiotics prescribed. Percentage of encounters with an injection prescribed A total of 8 (0.8 %) of the prescriptions had at least one injection prescribed along with other drugs. Percentage of drugs prescribed from the national essential drugs list Most of the medicines (95.4 %) were prescribed from the Nigerian Essential Drugs List. Extent of potentially inappropriate medicines Of the 1000 prescriptions studied, 456 (45.6 %) had one or more potentially inappropriate medicines from Beers’ list. This accounted for 601 (15.1 %) of all the medicines prescribed. The average age of those affected was 69.3 ± 6.9 years, 269 (58.9 %) of whom were women. Of those in the 60 -69 years age group, 285 (62.5 %) were mostly affected. Three hundred and thirty five (73.5 %) of the potentially inappropriate prescriptions had a single drug on Beers’ List. One hundred and twelve (24.6 %) of the prescriptions had two different medicines of concern (methyldopa and nifedipine) and 9 (1.9 %) had 3 -4 medicines from Beers’ List occurring concurrently. Table 3 shows the most commonly prescribed medicines in this study from Beers’ list, by generic name and severity of potentially adverse events. Medicines with high severity for potentially adverse events, including nifedipine, amitryptyline etc, occurred in 82.7 % of the cases while medicines with low severity for potential adverse events occurred in 17.3 % of the cases. Of the 456 prescriptions with one or more drugs from Beers list, 143 (31.4 %) had nifedipine occurring alone or in combination with other drugs such as amitryptyline and methyldopa. Nifedipine accounted for nearly a quarter (23.8 %) of the Discussion This study revealed the use of many therapeutic groups among the elderly. Analgesics were the most frequently prescribed, with ASA ranking as the highest of them. This finding is similar to those of other studies which also indicated that analgesics were the most prescribed medicines although these studies were based on palliative care [15-16]. The use of analgesics in the elderly is usually due to complaints of body pains by this special population. In addition to its analgesic effect, ASA was prescribed for its cardioprotective properties. Vitamins and minerals were the second most prescribed medicines. The high occurrence of vitamins and other health supplements in the prescriptions is not surprising as most people do not consume an optimal amount of all vitamins by diet alone. Pending strong evidence of effectiveness from randomized trials, it appears prudent for adults to take vitamin supplements. Physicians should make specific efforts to learn about their patients’ use of vitamins to ensure that they take only the vitamins that they should [17]. Antihypertensives were highly prescribed too, indicating a high occurrence of hypertension in this population. The frequency of antimalarials in the prescriptions (3.2 %) was low. This is contrary to expectations considering the fact that the study location is endemic for malaria; on the other hand, these patients probably indulge in self-medication whenever they suffer malaria attack since antimalarials are available over the counter in retail pharmacy outlets. Based on WHO prescribing indicators, some of the prescribing practices encountered in this study fell short of standard requirements. For instance, the number of medicines per prescription was found to be higher than the recommended range of 1.6 -1.8. Such high values have been found in previous Nigerian medicines use studies [12,18]. This may result in problems such as patients taking more medicines than their body systems can cope with, non-adherence to treatment regimen and therapeutic failure, e.g., from drug-drug interaction. Less than half of the medicines prescribed were generics. This finding is similar to those of previous studies [12,18] but falls short of WHO recommendation of 100 %. This implies that the prescribers are not complying with this recommendation although a majority of the drugs in Nigeria’s essential drugs are listed in their generic names. Prescription of medicines in their brand names often result in increased cost to the patient which may in turn lead to non-adherence to the prescribed drugs. It is worth noting that prescribing of antibiotics fell within the WHO recommended range of 20 – 26, while prescribing of injections was lower than the recommended range of WHO( 13.4 – 24.0 %). A lower rate of injection prescribing (7.5 %) has also been reported by Akande and Ologe [12]. Both differ from the finding of Aghaji where prescribing of injectables was 26.9 % [19] . Of great importance is the occurrence of inappropriate prescribing among the elderly observed in this study. Almost half of the prescriptions met Beers’ criteria for inappropriate prescribing in the elderly. Previous studies [3,20,21] also recorded potentially inappropriate medications though the level of occurrence is less than that found in our study. This and other studies [3,20-21], all point to one fact: inappropriate prescribing represent an important health problem for elderly patients and a major challenge for health practitioners. The reasons for inappropriate prescribing may be partly due to the relatively weak evidence-based guidelines for appropriate prescribing in elderly patients and existence of particulars justifying exceptions to the rules in individual patients [4]. Inappropriate medication use in patients 65 or older has been linked to many adverse drug reactions, poor physical functioning and excess healthcare use [22]. Interventions could target more appropriate drug selection by physicians when prescribing drugs such as short-acting nifedipine, methyldopa, amitryptyline, etc, to elderly patients as these were the most inappropriately prescribed medicines. Incidentally, amitryptyline was also found to be inappropriately prescribed in an earlier study, along with chlopropamide, propoxyphene and dypyridamol [21]. Interestingly, women and patients in their ‘sixties’ were the most at risk. This could be related to their being the modal gender and age, respectively, and therefore, interventions should be targeted to these groups. Limitations The results reported here are subject to some limitations. The study may not be totally generaliazable to all elderly since it was conducted using prescriptions of elderly persons attending outpatient clinics and did not include in-patients and other elderly people in the area. Conclusion Prescribing for the elderly was found to be suboptimal and there was occurrence of inappropriate prescribing. This calls for caution on the part of prescribers and pharmacists alike and also the need for awareness of tools that can be used by practitioners for detecting drug therapy problems. More studies are required on the pattern of inappropriate prescribing over a long period of time and on intervention programs to reduce potentially adverse health outcomes in elderly patients most at risk in the area where this study was undertaken. References
© Pharmacotherapy Group, Faculty of Pharmacy, University of Benin, Benin City, 300001 Nigeria The following images related to this document are available:Photo images[pr11004t3.jpg] [pr11004t1.jpg] [pr11004t2.jpg] [pr11004f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}