 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
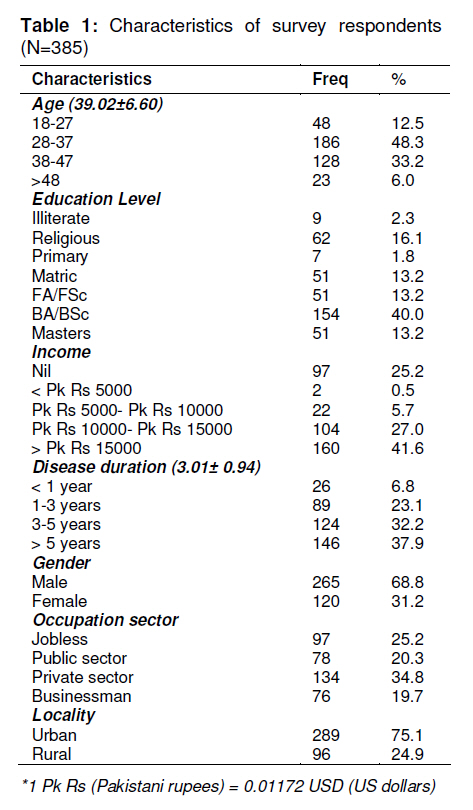
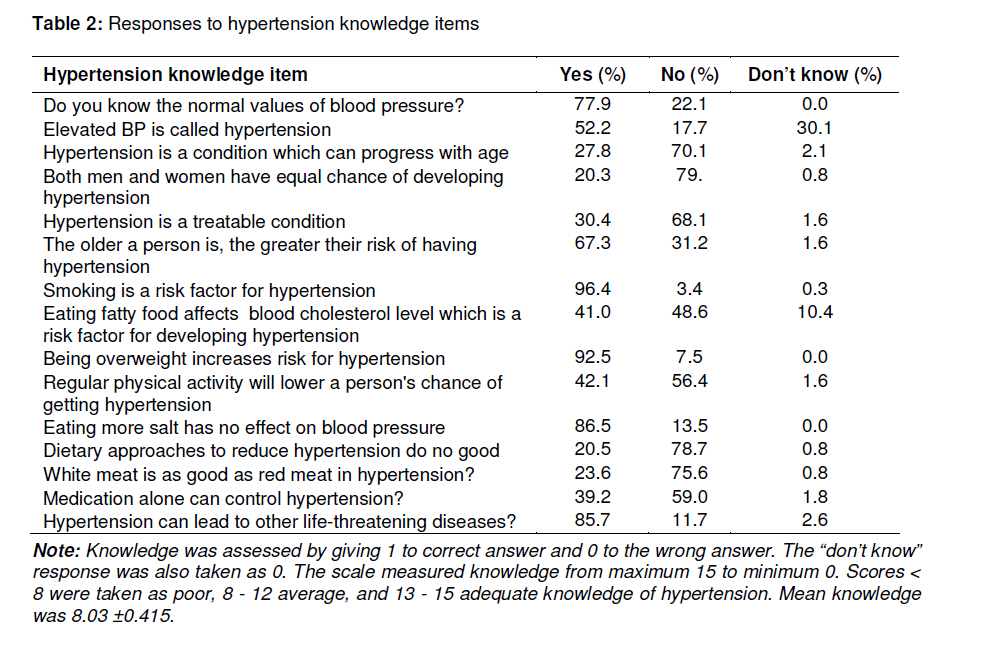
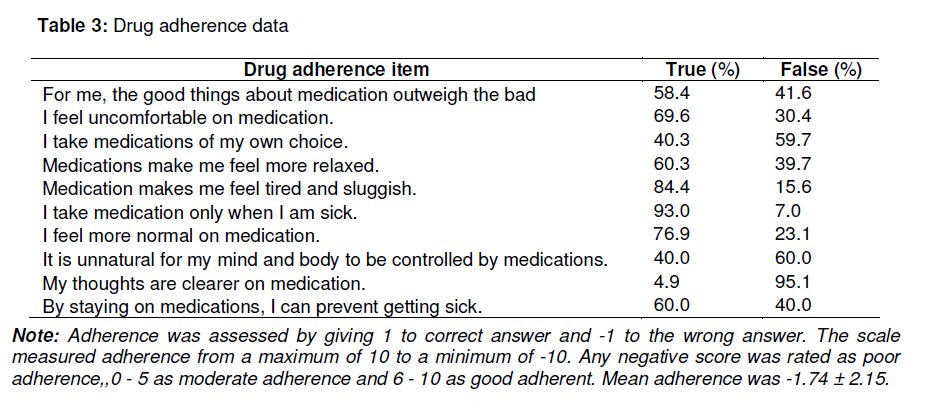
Tropical Journal of Pharmaceutical Research, Vol. 10, No. 2, April, 2011, pp. 125-132 Research Article Association between Knowledge and Drug Adherence in Patients with Hypertension in Quetta, Pakistan F Saleem1*, MA Hassali1, AA Shafie1, AG Awad2 and S Bashir3 1Discipline of Social and Administrative Pharmacy, School of Pharmaceutical Sciences, Universiti Sains Malaysia, 11800 Minden, Penang, Malaysia; Received: 6 August 2010 Revised accepted: 12 January 2011 Code Number: pr11018 Abstract Purpose: To evaluate the association between patient’s knowledge of hypertension management and medication adherence. Keywords: Knowledge, Drug adherence, Hypertension, Correlation. INTRODUCTION Hypertension is a major global concern and is one of the key preventable risk factors for cardiovascular events. It has massive disturbing impact on the population’s health, resulting in unnecessary morbidity and mortality. Hypertension alone is held accountable for more than 5.8 % of death worldwide, loss of 11.9 % year of life and adjusted life of 1.4 %. The assessment, management and control of hypertension still carry a great challenge for health care researchers [1]. Within the context of hypertension management, a number of factors are targeted as influencing agents but non-adherence to treatment is still counted as one of the major contributing factors to poor management and control of hypertension. Adherence has multiple definitions but the essence remains the same in every statement. It is “the extent to which patients stay with the recommendations of health care professionals” [2]. Sometimes, compliance and concordance are also used for the same purpose but have been replaced, as adherence focuses on patients and follows an active approach. While focusing on chronic diseases in general and hypertension in particular, these recommendations include instructions about continuous use of medication, life style modification, home monitoring and self-assessment [3]. Being a decisive component in achieving success of therapy, adherence to antihypertensive medication has been a topic of interest for health care researchers [4,5] and based on the results and conclusions, various approaches have been developed and implemented [6]. A number of studies highlighted multiple issues in non-adherence, including knowledge about hypertension by patients towards hypertension; the outcomes are not encouraging as far as adherence to medication is concerned [7]. The major population burden of the world is carried by Asia where the frequency of cardiovascular risk is also on the high side [8]. Very low degree of knowledge about hypertension and other cardiovascular conditions in the continent has often been reported [9]. Adequate data are not available on the extent of knowledge about hypertension and risk factors amongst Pakistanis, especially in those areas where incomes are low, including tribal areas, and among persons with no formal education and lack access to health facilities. Hypertension affects 23 % of the population, 18 % of persons aged > 15 years and 33 % of adults aged > 45 years [10]. Thus, the disease is emerging as a major clinical and public-health problem in Pakistan. Another study revealed that 18 % of the people in Pakistan suffer from hypertension with every third person above 40 years of age becoming increasingly vulnerable to a wide range of diseases, including myocardial infarction, stroke, atrial fibrillation, heart failure and renal failure. It was also mentioned that only 50 percent of the people suffering from hypertension were diagnosed and that only half of those diagnosed were ever treated. Half of those treated for hypertension were prescribed correct medication to effectively control the condition. Thus only 12.5 % of hypertension cases were adequately controlled [11]. At the same time, a large proportion of the population is unaware of their condition, which is alarming. Therefore, the objective of this study was to investigate the association between knowledge about hypertension and medication adherence amongst patients in Quetta City, Pakistan. METHODS Study design and recruitment of subjects A cross-sectional, observational study was employed as the method of data collection. Based on the prevalence of hypertension, a sample of 385 hypertensive patients was selected between the months of September 2009 and November 2009 from two tertiary care hospitals in Quetta, Pakistan, namely, Sandamen Provisional Hospital and Bolan Medical Complex Hospital. Both of these institutions carry the major population burden from all over the province of Baluchistan with a large proportion of low income patients. The inclusion criteria were: patients at least 18 years old, confirmed diagnosis of essential hypertension, those using antihypertensive agents for the last six months, and ability to speak and write in Urdu, the national language of Pakistan. The exclusion criteria were: patients aged < 18 and > 80 years, patients with co-morbidities, immigrants from other countries and pregnant women. Ethical issues As there was no human ethical committee for non-clinical studies in the said institutions, permission from the respective medical superintendents was obtained. Patients who agreed to participate were briefed on the nature and objectives of the study. Written and signed consent of the patients was obtained prior to data collection and this was followed by verification by the pharmacist working in cardiac units. The patients were assured of the confidentiality of their responses and their right to withdraw from the study with no penalty or consequences regarding their treatment. Data collection Two different questionnaires were used for the data collection. The Hypertension Fact Questionnaire (HFQ) was used to assess the level of knowledge and Drug Attitude Inventory (DAI-10) was used to measure the level of adherence of the hypertensive patients. Both instruments were pilot-tested with 40 established hypertensive patients for reliability and validity. The aim of the pilot study was to reveal difficulties in understanding the theme and meaning of the questions. Estimated amount of time of completion and willingness of the patients to participate in an interventional educational program was also taken into account. The data for patients involved in the pilot study was not taken into account in the main study. The instruments, originally constructed in English, were translated into the national language of Pakistan (Urdu) by a cardiologist with bilingual capabilities. It was made sure that the essential meanings of the items were preserved during translation. The translation was reconfirmed by a professor stationed at an academy of Urdu language. As the originality and consistency of the two instruments were stabilized, the final versions were reviewed and approved by the researchers. Little modification was necessary in order to improve comprehension by patients, but it was ensured that their original reliability and validity were retained. In addition to the two instruments, another form was also added to collect socio-demographic data that included age, gender, education, income, locality and duration of hypertension. Four pharmacists were trained to use HFQ and DAI-10 by the principal researcher and two cardiologists working in the respective hospitals. Focused group discussions were continuously held among the pharmacists, researchers and cardiologists to maintain the reliability of the data collection process. The data obtained were verified by the cardiologists and analyzed by the research team. Knowledge assessment tool HFQ, comprising 15 questions, was used to assess the knowledge of patients about hypertension, its causes, treatment and management. Each response was scored as ‘yes’, ‘no’ or ‘do not know’. The HFQ was constructed by the research team after extensive literature survey [12,13]. The scoring range of HFQ was 15 (maximum) to 0 (minimum). A cut off level of < 8 was considered as poor, 8-12 average, and 13-15 as adequate, knowledge about hypertension. Knowledge scores for individuals were calculated and and summed up to give the total knowledge score. Measurement of adherence DAI-10 (DAI) was used to measure the rate of drug adherence in the study patients. DAI consisted of 10 items with responses in the form of ‘yes’ or ‘no’, with scores ranging from 10 as maximum to -10 as minimum [14,15]. Patients scoring in the negative range were considered non-adherent, 0 -5 moderate adherent, and 6 -10 adherent. Data analysis Descriptive statistics were applied to compute the demographic and disease characteristics of the patients. All analyses were performed using SPSS version 16.0 (SPSS Inc., Chicago, IL). Spearman rank correlation test was used to measure the association between knowledge and drug adherence. RESULTS Patients’ demographics HFQ and DAI-10 were pilot-tested with 40 established hypertensive patients for reliability and validity (Cronbach ά = 0.70 for HFQ and 0.65 for DAI-10). The demographic characteristics of the study patients are presented in Table 1, including the frequency distribution of the study patients and diseaserelated data. The mean age of the patients was 39.0 ± 6.6 years, 68.8 % of whom were males. The mean duration of hypertension was 3.01 ± 0.94 years. Knowledge scores Table 2 describes the responses of the patients to HFQ in descending order. The HFQ scores ranged between 0 and 15. Overall mean score was 8.03 ± 0.42 and median score 8. Out of the 385 patients 146 (37.9 %) were within the poor knowledge range, 236 (61.3 %) moderate and only 3 patients (0.8 %) showed adequate general knowledge about hypertension. Poor knowledge was apparent in responses to questions relating to onset and management (questions 3 and 5) and dietary control of hypertension (questions 11, 12 and 13) where correct answers to these questions were 27.8, 30.4, 13.5, 20.5 and 23.6 %, respectively. Correct answers, 96.4, 92.5, 85.7 and 77.9 %, were highest in response to questions 7, 9, 15 and 1, respectively. Adherence scores The responses of the patients to DAI-10 scale are provided in Table 3. The DAI-10 test scores ranged between 10 and -10 with the overall mean score -1.74 ±2.154 and median score -2. Out of the 385 patients 249 (64.7 %) were categorized as poor adherent and 136 (35.3 %) as moderate adherent to their therapies. No patient was considered good adherent. Poor adherence was apparent in responses to questions 9, 5 and 2 where correct answers constituted 4.9, 15.6 and 30.4 %, respectively. Correct answers, 93.0 and 76.9 %, were highest in response to questions 6 and 7, respectively. The Spearman Rank order correlation coefficient between total score of knowledge and total adherence was – 0.170 (p < 0.001) DISCUSSION Hypertension is the most prevalent noncommunicable disease in the society but sadly, control of the disease is suboptimal. Although the patients had average knowledge about hypertension, the level of adherence was poor. In the context of the Pakistani population, the effect of knowledge possessed by the patients on drug adherence is still uncertain as there was no previous study in the same area that can be compared with the present study. However, studies undertaken in some developed countries indicate mixed responses. In the present study, knowledge had inverse relationship to drug adherence, suggesting that there are other factors for the patients’ non-adherence which need to be explored. There is evidence that knowledge or information can indeed have an influence on the level of drug adherence. A number of studies support such an association in which a positive relationship was found between knowledge and adherence [16,17]. Studies that measure determinants in successful drug adherence do portray knowledge as one influencing factor in achieving good adherence to therapy [18]. In certain cases, knowledge is again highlighted to be associated with adherence but only under certain conditions and circumstances [19]. In contrast, there are also studies that found no association [20]. The apparent reason for the conflicting outcomes and opinions may be due to differences in the concept and definition of adherence and knowledge. Sometimes, the effect of other factors cannot be discounted too. Since adherence is a multi–factor phenomenon, success or failure of therapy is not dependent on a single factor. Other factors such as age, gender, low socioeconomic status, prescribed drugs, posology, lack of social support, poor patientprovider relationship, cost, forgetfulness, and presence of psychological problems (especially depression) should also be kept in mind and evaluated before coming to a conclusion [21]. In the broader context of achieving optimal pharmaceutical care, one aspect stresses patients’ own understanding of disease, nature, management and treatment. This maximizes opportunity to exercise better control over the disease condition. In our case, a large proportion of the patients did not have a clear understanding of the disease they were suffering from, and had little information on treatment and management of hypertension. There is no established process of collaborative patient care as the key players in the health care system still bicker over roles and responsibilities, a situation that has adversely affected patient care services. Thus the interaction of the patient with the health care professional is rather limited which is probably one reason for poor adherence. It is high time that a patient-centred approach is adopted whereby the patient is involved in decision-making about his/her health. Another aspect of patient care revolves around the Health Belief Model which states that attitudes and beliefs of individuals can explain health behaviour [22]. In this model, perceived benefits and barriers in the health care regimen play a vital role in achieving therapeutic success. In our study, patients were seen making independent assessments of their disease, including its treatment and management, and were using different health systems (Ayurvedia and allopathy). This could be another reason for non-adherence to medication as multiple opinions from different health system alternatives as well as spiritual healers can complicate issues for the patient. Although some of the systems are not approved by the official authorities, their influence is pronounced in the population. The results notwithstanding, it is important that the patient should be educated on all aspects of the phenomenon rather than on a single or a few issues. It should also be addressed by social and medical researchers foregoing achieve a fuller understanding of the underlying issues while the outcome of such studies should be utilized in policy and decision-making by government officials and members of the health care team. Limitations of the study One possible limitation of this study is that it may appear as an observational study on outpatients in public hospitals that are usually attended by low to middle income and uneducated population. The high income and educated group also utilizes the health facilities but usually in cases of emergency; at other times, they attend private health facilities. Thus, the results of our research may not represent an accurate picture of the entire population. CONCLUSION Success of therapies is dependent upon the level of medication adherence carried out by patients. It is often believed that knowledge is one key factor in achieving better adherence. However, knowledge had an inverse relation in our cohort. It was also observed that patients had confusing perception of drug usage. Health care professionals can play a major role in this regard and a collaborative care approach should facilitate the education of patients about the benefits of medications and the importance of continuous medication use especially in the treatment and management of chronic diseases. Further studies are also recommended to identify the major contributory factor to non-adherence. CONFLICT OF INTEREST The authors declare no conflict of interest, in part or whole. No funding was received for this study. ACKNOWLEDGMENT The authors wish to thank the patients for participating in the study, and the hospital practice staff for their support. REFERENCES
Copyright © 2011 - Pharmacotherapy Group, Faculty of Pharmacy, University of Benin, Benin City, 300001 Nigeria. The following images related to this document are available:Photo images[pr11018t3.jpg] [pr11018t2.jpg] [pr11018t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}