 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
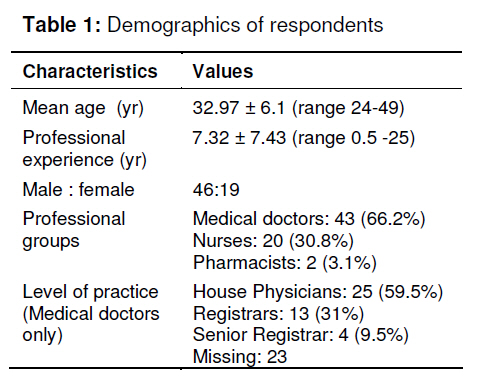
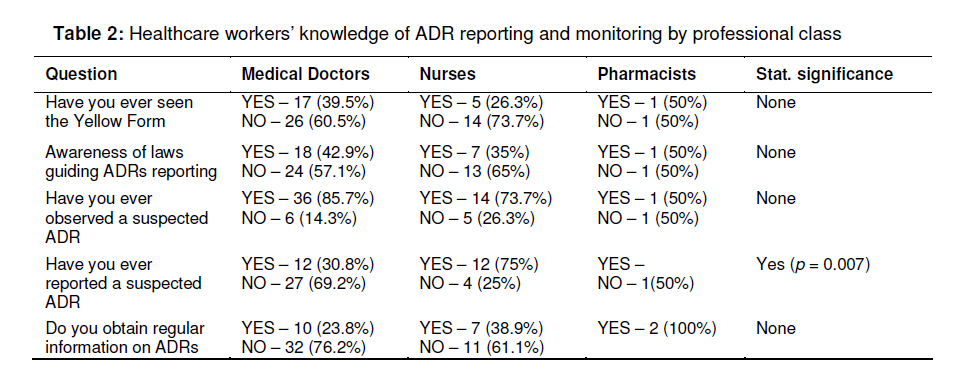
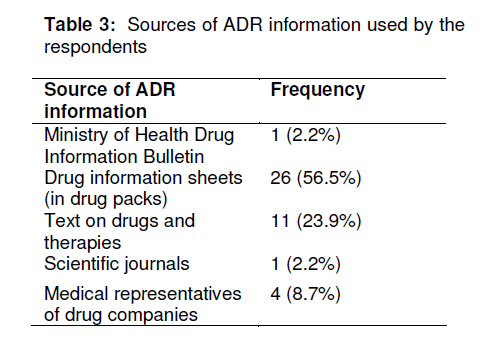
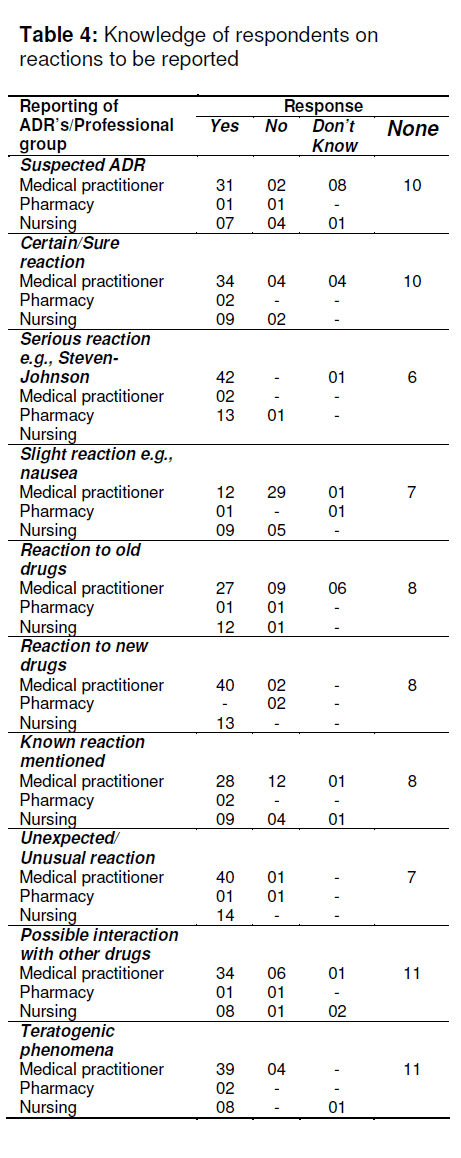
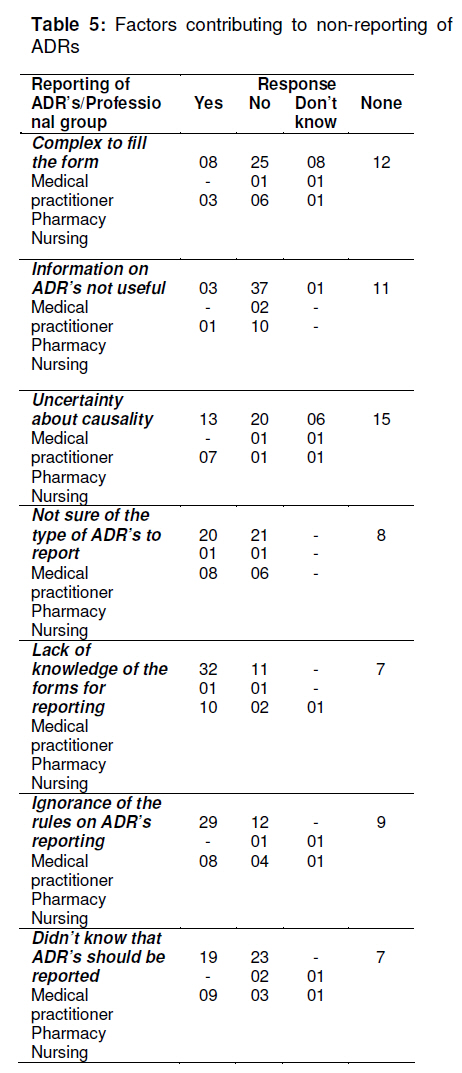
Tropical Journal of Pharmaceutical Research, Vol. 10, No. 3, June, 2011, pp. 235-242 Research Article Knowledge, Attitude and Practice of Adverse Drug Reaction Reporting among Healthcare Workers in a Tertiary Centre in Northern Nigeria Joseph O Fadare1*, Okezie O Enwere2, AO Afolabi3, BAZ Chedi4 and A Musa4 1Department of Medicine, Kogi State Specialist Hospital, Lokoja, 2Department of Medicine, Evans Enwerem University, Owerri and Imo State University Teaching Hospital, Orlu, 3Department of Surgery, Kogi State Specialist Hospital, Lokoja, 4Department of Pharmacology, Faculty of Medicine, Bayero University, Kano, Nigeria Received: 24 August 2010 Revised accepted: 22 April 2011 Code Number: pr11031 DOI: 10.4314/tjpr.v10i3.4 Abstract Purpose: To determine the knowledge, attitude and practice of ADR monitoring and reporting among healthcare workers in a teaching hospital in Kano, Nigeria Keywords: Adverse drug reactions; Knowledge, attitude and practice; Health care workers; Yellow card reporting scheme INTRODUCTION Adverse drug reactions (ADRs) are an important cause of morbidity and mortality worldwide [1]. According to World Health Organization (WHO) definition, an ADR is any noxious, unintended, and undesired effect of a drug, which occurs at doses used in humans for prophylaxis, diagnosis, or therapy [2]. The socio-economic and health consequences of ADRs have been highlighted in several studies [1,3,4]. While a majority of the studies cited above show prevalence of this problem in developed countries, there is paucity of accurate data from many developing countries. Out of the several methods of detecting ADRs, spontaneous reporting is one that has contributed significantly to improved levels of pharmacovigilance in many countries [5,6]. The importance of healthcare workers in the area of spontaneous reporting of ADRs and development of ADR databases worldwide has been established in previous studies [7,8]. Previous studies from different regions in Nigeria have concentrated on the perception and practice of ADRs reporting among physicians only while excluding other cadres of healthcare workers [9-11]. It is clear, however, that nurses and pharmacists have very important roles to play in ADR monitoring and reporting [12,13]. Despite the better ADR reporting culture of the developed nations, under-reporting is a major issue with spontaneous reporting [14,15]. The predictors of under-reporting have been described severally by many workers [16-18] but these differ from study to study. The objective of this study was to determine the knowledge, attitude and practice of ADR monitoring and reporting among healthcare workers (medical doctors, nurses and pharmacists) in a teaching hospital in Kano, Nigeria. METHODS Setting This study was conducted at Aminu Kano Teaching Hospital, Kano in northwestern part of Nigeria during the month of April 2008. It is one of the major tertiary health facilities in the area, providing medical and other ancillary services to about 10 million people, and also provides postgraduate training to resident doctors. It has four major clinical units, namely, Internal Medicine, Surgery, Paediatrics and Obstetrics and Gynaecology. Study design The study was a cross-sectional questionnaire-based study involving medical doctors, nurses and pharmacists working in different departments of the hospital. A convenience sampling method through which the questionnaires were distributed to the participants during their departmental activities was applied for the study. The sampling frame consisted of one hundred and sixty doctors (80 residents, 60 interns and 20 consultants) from the four clinical specialties, eighty nurses and twenty pharmacists servicing the needs of the teaching hospital. A sample size of one hundred and ten was considered proportionate and representative of this sampling frame. The questionnaire was adapted from a similar study investigating the attitudes and practice of ADR reporting among physicians in Nigeria [9]. It was designed to capture the following information: bio-data of respondents, professional group (medical doctors, pharmacists, and nurses), duration of practice, level of practice (e.g., interns, registrar), information about the knowledge and practice of ADR reporting, factors that may likely affect their reporting of ADR and suggestions towards a better ADR reporting culture. Data collection A total of 110 questionnaires were distributed to medical doctors (60) through chief residents of clinical departments; to nurses (40) through the Chief Nursing Officers of the respective wards and to pharmacists through the Assistant Chief Pharmacist. A time frame of one week was allowed for the collection of the anonymously filled forms. The completion of the questionnaire by respondents was taken as their consent to participate in the study. All cadres of medical doctors (consultants inclusive) had the questionnaires distributed to them and there was no deliberate plan to exclude any particular class. The absence of any cadre of doctors in the analysis could be due to their not returning the questionnaire within the stipulated time. Data analysis Information from the returned questionnaire was coded and entered into SPSS version 12 software. The results are presented as mean ± standard deviation, counts and percentages. The relationship between the different professional classes, duration of practice and their knowledge and practice of ADR reporting were determined using Chisquare at p < 0.05. RESULTS Only sixty-five respondents filled and returned their questionnaire within the stipulated time frame giving a response rate of about fifty-nine percent (59.1%). The demographics of the respondents, distribution by professional cadre and experience are shown in Table 1. Table 2 shows that a majority of the respondents (93.8 %) agreed that adverse drug reactions are an important cause of morbidity and mortality in medical practice. Regarding laws guiding the reporting of adverse drug reactions, eighteen of the medical doctors (42.9 %) and seven nurses (35%) were aware of their existence. The standard yellow reporting form for adverse drug reactions was only known to 39.5%, 26.3% and 50% of the participating doctors, nurses and pharmacists respectively. It is interesting to note that while over eightyone percent of the respondents had observed at least an episode of adverse drug reaction, less than half (42.7 %) of them had ever reported it. The main method of reporting found in this study was verbal and the report was made to a member of the managing medical team in over seventy-five percent of cases. The result also showed that a larger proportion (75%) of the nurses had reported at least a case of ADR as opposed to the medical doctors (30.8%) and that almost all the nurses put their report in the nurses report book. Table 3 shows the sources of ADR information used by the respondents. Less than half of the respondents (44.6 %) were aware of the hospital’ pharmacovigilance committee. Regarding the kind of reaction to be reported, a majority (> 70 %) of the respondents were aware that suspected, serious and certain reactions should be reported. Other types of reactions that should be reported according to the respondents are: reactions to new drugs, those mentioned in literature, unusual/unexpected reactions, possible interaction with other drugs and teratogenic reactions (see Table 4). The respondents identified the following factors as contributing to their non-reporting of ADRs: ignorance of the rules and procedures of reporting (66.1 %), lack of knowledge of the forms for reporting (74.1 %) and of what constituted ADRs (48.3 %). These and other factors contributing to nonreporting are shown in Table 5. The study also showed that the type of practice (medical or nursing) did have statistically significant effect on the reporting of adverse drug reactions (See Table 4). DISCUSSION The fact that majority of respondents agreed that ADRs are an important problem in medical practice is an encouraging finding from our study. Our earlier reported finding of lack of knowledge of the yellow reporting forms by majority of the respondents is in line with similar studies in Nigeria [9-11]. The reason for the similarities among different geographical regions of Nigeria could be due to inadequate attention to the subject of ADRs in the clinical pharmacology and therapeutics curricula of medical schools. This common observation about lack of knowledge about the yellow forms could also indicate that under-reporting of ADRs is a major issue in Nigeria with its attendant consequences. Some studies in the USA and France [2,3] had shown that ADRs contribute significantly to morbidity and mortality in clinical practice with its associated economic consequences. It seems that the situation in Nigeria may not be very different and the problem is unrecognized due to gross underreporting. Under-reporting of ADRs is a worldwide phenomenon and this has been established from previous studies [14,15,19,20]. The determinants of under-reporting, from our study, include lack of knowledge of the forms for reporting, ignorance of the rules and procedure for reporting, and not being sure of the type of reactions to be reported. This tallies, to a large extent, with other reports from Nigeria, China and Malaysia [9,18,21]. While it is important to note that these studies were carried out among physicians, several other studies involving pharmacists have indeed confirmed that under-reporting of ADRs is common to all health care professionals [22,23]. It is also interesting to note the non-response of medical consultants and the low level of participation by pharmacists in this study. This outcome could be a reflection of the importance attached to the problem of ADRs by this category of medical personnel and this is not very encouraging. A similar study carried out in Ibadan [9] also included only residents; this raises questions about the accessibility of medical consultants for such important studies. Our study included some nurses because of their primary importance in the care of patients, especially patients on hospital admission. Because nurses are in the ward at all times, it is most likely that any acute adverse drug reaction will first be observed by them, hence it is important that they participate in the spontaneous reporting scheme. In countries where nurses are already participating in the ADR reporting scheme, studies have shown that they indeed contribute positively towards the promotion of ADR reporting [7,24]. In this study, a majority of the nurses reported some form of ADR through the nurses daily report book and not the yellow card reporting scheme. This finding highlights the important role nurses can play if they are properly trained in the area of pharmacovigilance. It is a known fact that information regarding ADRs changes on a daily basis and hence the need for constant updating of the knowledge of health care professionals in this area. Most respondents in this study obtained their information on ADRs from drug information sheets and texts on drugs. Lack of, or inadequate, access to the internet can be a major limiting factor (where internet facilities are poor) for obtaining current reports on ADRs as most information from drug inserts and textbooks on drugs may be outdated and may not reflect the current state of information on ADRs. In order to address some of the determinants of under-reporting found in this study, ADR reporting guidelines should be made available in the form of booklets and posters at conspicuous locations in health care facilities to serve as a constant reminder. This should be in addition to regular sensitization of all health care workers on the importance of pharmacovigilance in the quest to decrease morbidity and mortality among the populace. Some workers have suggested the use of financial incentives as a tool to stimulate reporting of ADRs [25]. Apart from the fact that the use of incentives have not been widely accepted and practiced, it raises the possibility of over-reporting by some health care workers in a bid to obtain financial rewards. This should not be supported because ADR reporting should be a fundamental responsibility of health care workers and, therefore, it should be understood as such. Improving ADR reporting, apart from reducing the incidence of adverse drug reactions in clinical practice, will also lead to a reduction in health care costs. Another way to increase the reporting of ADRs is through the promotion of patient self-reporting. The benefits of this idea have been confirmed in different studies [26,27]. Patient self-reporting has a complimentary role to play in increasing the level of ADR reporting in a developing country such as Nigeria. Although Nigeria’s regulatory agency, National Agency for Food and Drug Administration Control (NAFDAC), has been doing a lot of sensitization through the media regarding the issue of ADR reporting, efforts should also be made to make the reporting process by patients simple and straightforward. The lack of awareness of the availability of pharmacovigilance committee in the Aminu Kano Teaching Hospital, Kano by more than half of the respondents indicates the need to extend the level of sensitization for health care workers to improve their ADR reporting. Limitations of the study The main limitation of our study was the relatively small number of respondents, especially pharmacists. In addition, some other factors that are associated with selfreporting studies such as accuracy of recall, personal bias and could also have affected, in some ways, the results of this study. The opinion of non-responders in general and participants who did not respond to certain aspects of the questionnaire could also have affected the interpretation. CONCLUSION Adverse drug reaction reporting using the Yellow Card reporting scheme is low among health care workers (doctors, nurses and pharmacists) at the Aminu Kano Teaching Hospital, Kano, Nigeria. There is a need for regular training and re-enforcement of guidelines for ADR reporting among health care personnel. Yellow card ADR reporting by nurses and patient self-reporting should also be encouraged. ACKNOWLEDGEMENT The authors would like to thank the members of staff of the Aminu Kano Teaching Hospital who participated in this study. Special thanks to Dr Garba Iliasu who took charge of the distribution of the questionnaires. COMPETING INTERESTS None REFERENCES
Copyright © 2011 - Pharmacotherapy Group, Faculty of Pharmacy, University of Benin, Benin City, 300001 Nigeria The following images related to this document are available:Photo images[pr11031t2.jpg] [pr11031t1.jpg] [pr11031t4.jpg] [pr11031t5.jpg] [pr11031t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}