 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pharmacology & Therapeutics, Vol. 1, No. 1, 2002, pp. 12-16 Paediatric Premedication: A Comparison of Sublingual Buprenorphine and Midazolam in Children (4-10 Years) Scheduled for Adenotonsillectomy VALIOLAH HASSANI, AKRAM AMANNI, MOHAMMAD POURESLAMI, and SOODABEH DJALALI MOTLAGH Department of Anesthesia, Rasool-e-Akram Hospital
(V.H.),Department of Anesthesia, Shahid Rajaee Hospital (S.D.M.) and Department
of Statistics (M.P.), Iran University of Medical Sciences, Tehran, Iran;
Pasteur Institute of Iran, Tehran, Iran (A.A.) Received May 20, 2002; ABSTRACT Introduction and Objectives. Preanesthetic
medication may reduce the risks of adverse psychological and physiological
sequela of induction of anesthesia in children. Administration of premedication
by sublingual route may provide the best compromise, that is, relatively rapid
absorption without causing pain. In this study, we compared sedative and anxiolytic
effects of midazolam and buprenorphine in children. Keywords: anesthesia, sublingual premedication, benzodiazepine, opioid, adenotonsillectomy Surgery and anesthesia induce considerable emotional stress in both parents and children [1]. The consequences of this stress may remain long after the hospital experience has passed, including prolonged night terrors, negativism, a variety of phobias, hysterical reactions and anxiety reactions [2]. Preanesthetic medication may reduce the risks of adverse psychological [3] and physiological [4] sequela of induction of anesthesia in a distressed child. Premedication may be administered orally, intramuscularly, intravenously, rectally, nasally or sublingually. Although most of these routes are effective and reliable, each has drawbacks as well. Sublingual medications may provide the best compromise, that is, relatively rapid absorption without causing pain [5]. Karl et al. have demonstrated that sublingual administration is an effective route of midazolam administration for premedication in children [6]. Since buprenorphine has the most effective sublingual absorption in comparison with many opioids studied [7], in this study, we compared sedative and anxiolytic effects of sublingually administered buprenorphine and midazolam as preanesthetic medication in children. Methods After approval by the university research committee and obtaining parental consent, in this placebo-controlled, randomized, double-blinded, clinical trial, one hundred and fifty normal healthy children, aged between four and ten years scheduled for adenotonsillectomy were enrolled. Exclusion criteria included: a previous general anesthetic, current opioid or sedative medication, airway problems, upper respiratory tract infection, or children who spat out or early swallowed the premedicant. The children were assigned by random selection to one of the three following groups: group 1 (50 patients) received buprenorphine 3μg/kg sublingually an hour before the scheduled surgery time. Those in group 2 (50 patients) received midazolam 0.2 mg/kg sublingually mixed with 0.2 ml apple juice, and those in group 3 (50 patients) received no premedication but to prevent unblinding the parents, they received 1 ml apple juice sublingually both of which 10 minutes before the expected time of induction of anesthesia. Drug preparation: Available buprenorphine preparation was 0.4 mg sublingual tablets, which was grounded and mixed with 2 ml sterile water. The resultant suspension contained 200 µg/ml buprenorphine. After taking appropriate dose of the drug for every child in an insulin syringe, the needle was removed and the syringe was tipped in apple juice and used. Because no sublingual preparation of midazolam was available, the parenteral preparation (5 mg/ml) was used. An anesthesia resident not involved in the management of patients or in gathering data for the study except for recording vital signs and was present in the operating room in case of any complication, gave each child the premedicant. Children were asked to place the tip of the tongue to the back of the upper teeth, and the premedicant was placed under the tongue. The child was told not to swallow; at 30 sec the child was permitted to swallow the drug. Children, who spat out or swallowed the medication before the 30 sec sublingual retention period, were excluded from further analysis. Heart rate, respiratory rate, and oxygen saturation (SpO2) were measured every five minutes from just before administration of the premedication to induction of anesthesia. Decrease in heart rate or respiratory rate by 20% or SpO2 below 95% was recorded. Sedation and anxiolytic levels were scored by the first observer blinded to the drug administered as premedication (one hour before induction), at separation of the child from his/her parents, and prior to induction of anesthesia. Sedation was measured on a four-point scale (1 = alert/active; 2 = awake/calm; 3 = drowsy but responds to verbal/tactile stimuli; 4 = asleep). Anxiolysis was also measured on a four-point scale (1 = tearful/combative; 2 = anxious but easily reassured; 3 = calm; 4 = asleep). Mask acceptance was recorded by the first observer on a four-point scale similar to that used by Feld et al. to assess mask acceptance [8] (1 = combative/screaming; 2 = crying but easily reassured; 3 = occasionally sobbing/mostly calm; 4 = peaceful). In order to prevent interobserver variability in scoring, only one observer blinded to the drug administered evaluated all 150 children. Induction of anesthesia was accomplished with inhalation of halothane (graded increments) in oxygen. A cannula was inserted into a peripheral vein; atropine 10-20 µg/kg I.V. and alfentanil 10 µg/kg I.V. were injected, before tracheal intubation. Anesthesia was maintained by spontaneous inhalation of halothane and nitrous oxide in 50% oxygen. All drugs were discontinued simultaneously at the end of surgery. The trachea was extubated when the gag reflex had returned. The times from discontinuation of anesthesia until extubation and spontaneous eye opening were recorded. Heart rate, respiratory rate, and SpO2 were measured every hour postoperatively. If the child fell asleep during the six-hour postoperative period, SpO2 was monitored continuously until s/he woke up again. Analgesia was provided by acetaminophen elixir 10 mg/kg every 6 hours. Side effects including apnea, airway obstruction, or vomiting within 24 hours postoperative period were noted. Before discharge from the hospital parents were asked to complete a questionnaire regarding their opinion about the premedication their child had been given. They were asked to rate their preoperative experience on a three-point scale (1 = excellent; 2 = acceptable; 3 = unacceptable/unpleasant). Data Analysis. Results were analyzed using analysis of variance for parametric data. In order to evaluate the sedative effect of the drug in each group, the proportion of children who were calm, drowsy, or asleep in each measurement period was compared with the proportion at baseline; for anxiolysis, the proportion of children who were calm or asleep at each measurement period was compared with the proportion at baseline both using Mac-nemar test. For sedation, anxiolysis, mask acceptance between groups, results were analyzed by Kruskal Wallis test. Nominal data (gender, incidence of vomiting) were analyzed using Fisher’s exact test. Results were considered significant at p < 0.05. Results There was no difference between the groups with respect to age, gender, weight, (Table 1), baseline sedation and anxiolytic scores, and duration of surgery (Table 2).
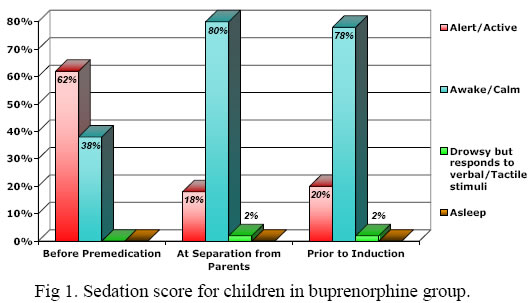
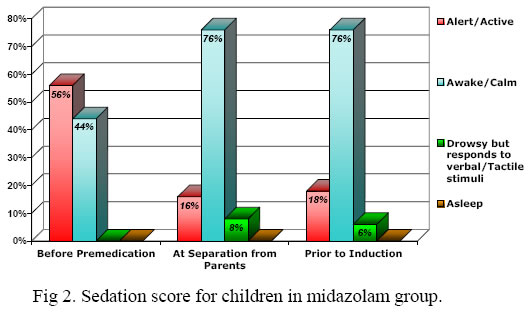
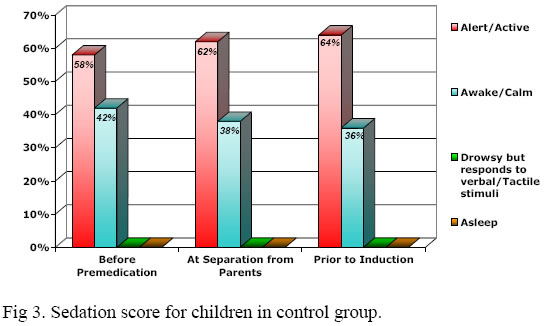
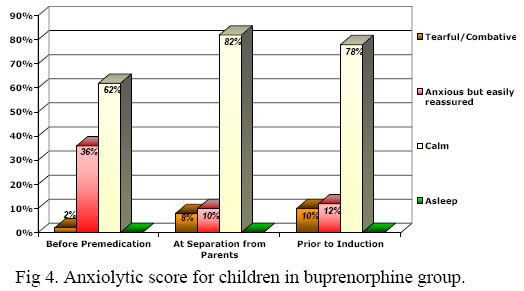
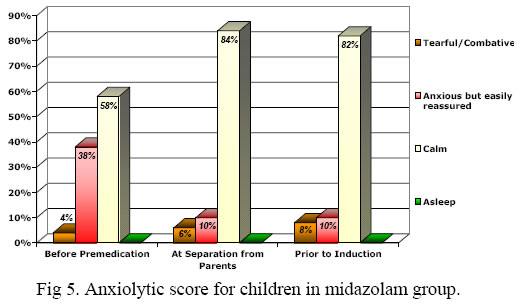
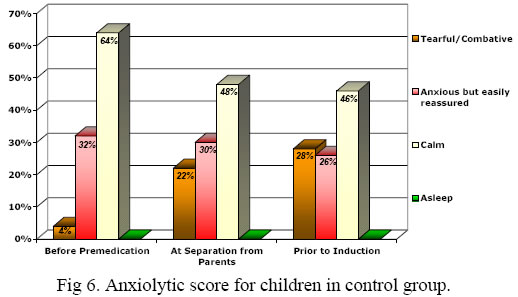
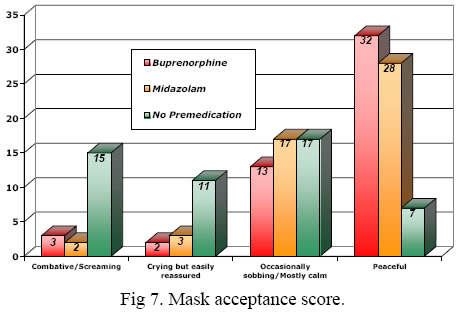
Six patients spat out their premedication (buprenorphine = 2; midazolam = 3; no premedication = 1), and four patients swallowed the premedication before 30 sec. (buprenorphine = 2; midazolam = 1; no premedication = 1). They were all omitted from further assessment. None of the children had SpO2 < 95% or over 20% decrease in heart rate or respiratory rate during the period between drug administration and induction of anesthesia. Sedation scores at separation of children from their parents and prior to induction of anesthesia were similar in groups 1 and 2, both of which were higher than group 3 (p = 0.00001; Figure 1, 2 and 3). The proportion of calm or drowsy children (sedation scores 2 & 3) in buprenorphine group at separation from parents (82%; p < 0.01) and prior to induction (80%; p < 0.01) were greater than the proportion at baseline (38%). In midazolam group, this proportion at separation from parents (84%; p < 0.01) and prior to induction (82%, p < 0.005) were also greater than that at baseline (44%). In contrast, in control group, the same proportion at separation from parents (38%; p < 0.001) and prior to induction (36%; p < 0.001) were smaller than that at baseline. With regard to anxiolysis (Figure 4, 5 and 6), anxiolytic scores at separation from parents and prior to induction were similar in groups 1 and 2, both of which were higher than group 3 (p = 0.0001). The proportion of calm children (anxiolytic score = 3) in buprenorphine group at separation from parents (82%; p < 0.001) and prior to induction of anesthesia (78%; p < 0.001) was greater than that at baseline (62%). The proportion of calm children in midazolam group at separation from parents (84%; p < 0.001) and prior to induction (82%; p < 0.001) was also increased in comparison to that at baseline (58%). But in control group this proportion at separation from parents (48%; p < 0.001) and induction of anesthesia (46%; p < 0.001) were decreased in comparison to that at baseline (64%). Mask acceptance (Figure 7) was better in patients of both buprenorphine and midazolam groups than the control group (p = 0.00001). Times from discontinuation of anesthesia until extubation (p = 0.0001) and spontaneous eye opening (p = 0.00001) were delayed in the midazolam group in comparison with the two other groups (Table 2). In the ward, none of the children experienced apnea, oxygen desaturation, or airway obstruction. Nineteen patients in group 1, twenty-four patients of those in group 2, and seventeen patients of those in group 3 had one or more episodes of emesis. Incidence of vomiting was similar in all groups. Parents whose children were given buprenorphine or midazolam where similarly satisfied and both had a higher satisfaction rating than parents whose children were not given premedication (p = 0.0001; Table 3). Discussion Transmucosal administration of premedicant has many advantages:
Midazolam has become the most commonly administered premedicant before routine surgery in many pediatric centers [1]. It has been administered by oral, [8, 11, 12, 13] nasal [9, 14], rectal, intramuscular (I.M.) [1] or sublingual routes [6, 15, 16]. Sublingual administration of midazolam (0.2-0.3 mg/kg) is as effective as intranasal route, but sublingual administration is associated with a better patient compliance [6]. Another concern with nasal midazolam is the theoretic possibility of neurotoxicity by drug transport along the neural connection between the nasal mucosa and the central nervous system through olfactory nerves [5]. Like other transmucosal routes of administration, sedation is achieved within 10 minutes [15], which is the reason we chose 10-min interval between drug administration and separation from parents. The sedation achieved is usually not sleep but rather a compliant happy state. If sleep occurs, a relative overdose has probably been given [5]; none of the children in this study fell asleep. Interest in the use of opioids as pediatric premedication has focused on the intranasal (e.g. sufentanil) and oral transmucosal (e.g. fentanyl citrate) forms of administration [1]. We studied buprenorphine here, because it has a greater sublingual absorption in comparison to some other opioids [7]. Buprenorphine is a thebaine derivative, µ-receptor partial agonist, and similar in structure to morphine but approximately 33 times more potent. Buprenorphine has been successfully used for premedication, as the analgesic component in balanced anesthesia and for postoperative pain control, and it has been administered sublingually, intravenously, epidurally, and rectally. Sublingual buprenorphine, given 1 hour preoperatively, provides reliable preoperative sedation and postoperative analgesia similar to I.M. morphine [5]. It has been used successfully for postoperative pain relief [17] and premedication in children [18]. The rich blood supply of the sublingual mucosa allows rapid absorption of drugs directly into the systemic circulation [6]. Since venous drainage from the mouth is to the superior vena cava, the drug is also protected from rapid first-pass metabolism by the liver [19]. Absorption depends on the time that the drug is adjacent to the mucosal surface (resident time), local pH (6-7.4), saliva flow, and physiochemical characteristics of the drug themselves and of the chosen site [6]. Lipid soluble molecules can diffuse easily across the cell membrane [19]. Midazolam is highly lipophilic. Its solubility is pH dependent, it is water soluble when the pH is below 4 and is lipid soluble when the pH is above 4 [5]. The midazolam preparation used in this study had a pH equal to 3.17 and when it was mixed with apple juice (pH = 3.30), the resultant pH of the solution was about 3.22. The drug may become lipid soluble in contact to sublingual mucosa (pH = 6-7.4) and can diffuse readily across mucosal membrane. Buprenorphine hydrochloride is a white powder, weakly acidic, highly lipophilic, and with limited solubility in water [19]. We mixed every sublingual tablet with 2 ml distilled water (pH = 7), to prepare appropriate dose for children. Since the rate of dissolution may be the limiting factor in drug absorption for drugs given in solid form [19], we possibly accelerated the drug absorption by mixing it with water. Karl et al. found a 10% incidence of crying at separation from parents after sublingual administration of midazolam as premedication [6]. In this study, 6% of patients in midazolam and 8% of those in buprenorphine group were tearful at separation from parents, but children in Karl’s study were younger (0.5-10 years). She classified the children into three age groups; eighty-eight percent of those in school-age group (5.1-10 years) had excellent or adequate behavior score at separation from parents. Although scoring in her study has been slightly different from our study, the results are comparable, and the results in this study are consistent with Karl’s report. In order to quantitate the speed of recovery, we recorded the time from discontinuation of anesthesia until a specific and objective end-point in recovery was achieved. Time from discontinuation of anesthesia to spontaneous eye opening was longer in midazolam group in comparison with the two other groups. It has been shown that cytochrome P450 3A4 activity is a significant factor in metabolism of both midazolam and alfentanil [20, 21]. Thus, prolongation of recovery time in midazolam group may be related to drug metabolism. Benzodiazepines and all µ-receptor stimulating opioids cause dose-dependent depression of respiration [5]. Karl et al. reported that 2% of children who received nasal midazolam and 54% of those who received nasal sufentanil as premedication had SpO2 < 96% [9]. In our study, none of the children in either group had SpO2 < 95% during the time from drug administration to 6 hours postoperatively. Because of pharyngeal mucosal irritation from surgery and bloody secretions that are swallowed, emesis is relatively frequent after adenotonsillectomy [1]. We used alfentanil at induction of anesthesia which can also increase the incidence of nausea and vomiting, but we believe that these two factors (type of surgery and use of an opioid during induction of anesthesia) affected all groups similarly and therefore comparing incidence of emesis in the 3 groups might be valuable. In conclusion, sublingual buprenorphine is as safe and effective as sublingual midazolam in providing sedation and anxiolysis for pediatric premedication. References
Copyright © 2002 by Razi Institute for Drug Research (RIDR) The following images related to this document are available:Photo images[pt02004f1.jpg] [pt02004f7.jpg] [pt02004f2.jpg] [pt02004f4.jpg] [pt02004f3.jpg] [pt02004f6.jpg] [pt02004f5.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}