 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pharmacology & Therapeutics, Vol. 4, No. 1, 2005, pp. 9-12 Hypolipidemic Activity of Ginkgo biloba Extract, EGb 761 in Hypercholesterolemic Wistar RatsARUN KUMAR DUBEY, AHALYA DEVI, GOPALAN KUTTY and RAVI PATHIYIL SHANKAR Department of Pharmacology, Manipal College of Medical Sciences, Pokhara, Nepal (A.K.D., R.P.S.); Department of Pharmacology, Kasturba Medical College, Manipal, India (A.D.); Department of Pharmacology, College of Pharmaceutical Sciences, Manipal, India (G.K.). Address correspondence to: Dr. Arun K Dubey, Department of Pharmacology, P.O. Box 155, Deep Heights, Pokhara, Nepal. E-mail: arundubey65@yahoo.co.in Received September 14, 2004; Code Number: pt05002 ABSTRACT Cardiovascular diseases are becoming an increasing problem worldwide. Hypercholesterolemia has been implicated in causation of coronary heart disease. Oxidation of low density lipoprotein has been shown to be prevented by standardized Ginkgo biloba extract, EGb 761. Studies on the effect of Ginkgo biloba on serum lipid levels are lacking. Hence the present study was carried out to study the effect of EGb 761 on serum lipids in female wistar rats. The hypolipidemic effect was compared with a standard dose of lovastatin. The rats were divided into six groups of ten animals each. The first group was the normal control. The second group was given cholesterol (400 mg/kg) for 30 days. The third, fourth and fifth groups were given cholesterol and EGb 761 in the doses of 25 mg/kg, 50 mg/kg and 100 mg/kg respectively. The sixth group was given lovastatin (7.2 mg/kg) in addition to cholesterol. Serum cholesterol, triglycerides and high density lipoproteins were measured on days 0, 15 and 30. Serum levels on days 15 and 30 were compared using students paired t-test (p < 0.05). There was a significant decrease in serum cholesterol in both the lovastatin and the EGb 761 treated groups. EGb 761 did not produce a significant change in serum triglyceride and high density lipoprotein levels. The animal model used had limitations and further studies are required. Keywords: Cardiovascular diseases, Ginkgo biloba extract, Hypolipidemic drugs, Serum Cholesterol Cardiovascular diseases with an incidence of approximately 50% are the main cause of death in most advanced countries [1]. The disease burden contributed by cardiovascular diseases has been increasing in the developing world also. The World Health Organization (WHO) estimates that every year 12 million people worldwide die from cardiovascular diseases, with most of them being from the developing world [2] . Most people would benefit from lowering their blood pressure and cholesterol level. The underlying primary cause of cardiovascular disease is believed to be atherosclerosis, a progressive mul tifactorial disease of the arterial wall [ 3, 4 ] . Central to the pathogenesis of atherosclerosis is deposition of cho lesterol in the arterial wall [ 5] . Nearly all lipoproteins are involved in this process including cholesterol carried by very low-density lipoproteins (VLDL), remnant lipoproteins and low-density lipoproteins (LDL). The most important study done to demonstrate that blood cholesterol is a risk factor for coronary artery disease (CAD) is the Framingham study initiated and operated by the National Heart, Lung and Blood institute, USA. Animal studies and many large, randomized double blind studies in human beings prove beyond doubt, the cause and effect relationship between hypercholes terolemia and morbidity and mortality from CAD [ 6, 7 ] . Hypolipidemic therapy is highly effective in reducing the risk as has been demonstrated dramatically in the Scandinavian Simvastatin Survival Study (4S) [ 8] . In addition, the past decade saw a series of remarkable studies that suggested oxidative systems, particularly oxidation of LDL is a risk factor and plays a role at several steps of atherosclerosis [9, 10]. A decrease in oxidative stress and protection of LDL from oxidation might therefore be a strategy with great promise for prevention of atherosclerosis associated cardiovascular disease [ 11]. The intense interest in this area stems in part from the generally low toxicity of antioxidants and the hope that treatment with antioxidants might be additive with cholesterol lowering regimes. Ginkgo biloba has been used in traditional Chinese medicine for over 5000 years.
The extract from the leaves of Ginkgo biloba is used today as a standardized preparation EGb 761 which contains 24% flavonoid glycosides, mainly kaempferol and quercetin, glucorhannoside esters and 6% terpenes, the ginkgolides and bilobalides [12]. The mixture of biologically active ingredients gives the whole extract a complex range of activities; for example, the flavonoids act as free radical scavengers and the terpenes, particularly ginkgolide B are potent inhibitors of Platelet Acti vating Factor (PAF) [13]. Ginkgo biloba extract has been shown to prevent LDL oxidation in the arterial wall, in certain animal and human studies [ 14] . Studies on the effect of Ginkgo biloba on the serum lipid level are lacking. Hence, the present study was carried out. The objectives of the study were to:
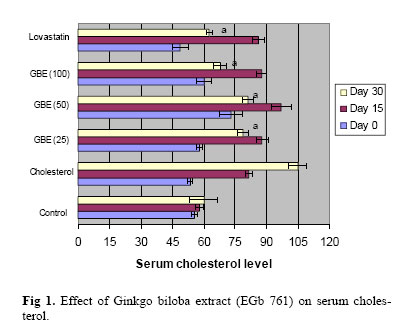
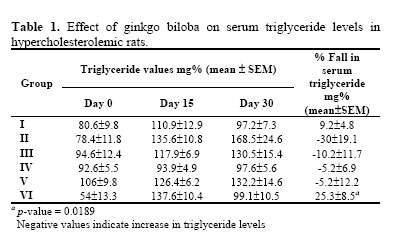
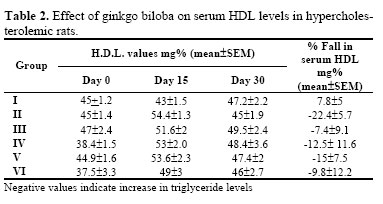
Animals Healthy, female, albino rats of Wistar strain, weighing 150-200 gms. bred in our animal house were used for the study. The animals were given standard rodent diet and water ad libitum throughout the study. The study was conducted in accordance with the internationally accepted principles for laboratory animal use and care as per the US guidelines (NIH publication No. 8523, revised in 1985). The study was conducted in the Department of Pharmacology, Kasturba Medical College, Manipal, India. Materials A. Pure Ginkgo biloba extract (EGb 761) was procured from German Remedies, Mumbai, India. B. Cholesterol extra pure for feeding purpose was obtained from Loba Chemie, Mumbai, India. Coconut oil was used as a vehicle for cholesterol feeding. C. Tablet lovastatin was obtained from Cipla Pharmaceuticals, Mumbai, India. Experimental Procedure All the animals were weighed and divided into six groups. There were ten animals in each group. All experiments were carried out between 10 am and 2 pm. Group I. Normal control. Carboxy methyl cellulose 0.25% w/v was used as the vehicle to administer EGb 761 and lovastatin. Cholesterol, EGb 761 and lovastatin were fed to the rats using a rat feeding tube. Biochemical Parameters Biochemical parameters measured in the study were serum cholesterol, triglycerides and HDL. The blood samples were collected from the orbital sinus of rats with the help of a capillary tube. Baseline investigations were done at the beginning of the study and then repeated at the end of 15 and 30 days for all the groups. The serum was stored in deep freezer and analyzed within 3 days. The estimations were made using Autoanalyser (Hitachi-911). The different reagents used for the estimation of serum cholesterol, serum triglycerides and HDL were procured from Boehringer-Mannheim Pvt. Ltd. Statistical Analysis Students t-test (GPIS software package) was used. A p-value of less than 0.05 was taken as statistically significant. The serum cholesterol, triglycerides and HDL levels on day 30 was compared to the levels on day 15 and the % fall was calculated. RESULTSHypercholesterolemia was produced in rats by feeding a high cholesterol diet. From days 15 to 30, three groups of rats were administered Ginkgo biloba extract (EGb 761) in three different doses (25 mg/kg, 50 mg/kg, and 100 mg/kg). The results were compared with the group of animals treated with lovastatin as well as two control groups, one group serving as normal control while the other group served as cholesterol control. All the animals were in good health throughout the study period and average body weight of the animals did not change significantly during the study. Serum cholesterol The baseline serum cholesterol values for the different groups were estimated on day 0. Repeat estimations were done on days 15 and 30. On day 15 control rats had a mean±SEM serum cholesterol level of 58.0±1.9 mg%. In the cholesterol control group (group II), the value on day 15 was 81.6±1.6 mg% showing a significant elevation from the normal value. The values measured on day 30 showed that there was a significant fall in serum cholesterol in both lovastatin and Ginkgo biloba treated groups. This is shown in Fig 1. Serum triglycerides On day 30 normal rats had a mean±SEM serum triglyceride level of 97.2±7.3 mg%. In the cholesterol control group this value was 168.5±24.6. Ginkgo biloba did not produce any significant fall in serum triglycerides ( Table 1). Lovastatin produced significant reduc tion in triglyceride levels. Serum HDL level Normal rats had mean±SEM serum HDL levels of 47.2±2.2 mg% on day 30. In the cholesterol control rats this value was 45.0±1.9. Effect on serum HDL level is shown in Table 2. There was no significant change in HDL values in any of the drug treated animals. DISCUSSIONThere was a significant decrease in serum cholesterol levels in all the Gingko biloba treated groups. However the fall in serum cholesterol was less than that of the group treated with lovastatin. The % fall in serum cholesterol values of Ginkgo biloba treated animals ranged from 9.51 to 16.31. For the group treated with lovastatin, the % fall was 26.4. As the dose of Ginkgo biloba increased there was an increase in the % fall in serum cholesterol values. However, the fall was not proportionate to the increase in the dose of Ginkgo biloba. Although lovastatin reduced triglyceride levels significantly, similar effect was not observed in the animals treated with Ginkgo biloba. There was no increase in HDL levels in either the Ginkgo biloba treated group or the group given lovastatin. This is in contrast to the studies that report slight increase in HDL levels with the statins [ 16] . Although Ginkgo biloba has been used in some countries as a hypolipidemic agent, there are no published reports in English, of its action on lipid profile [17] . Therefore it was not possible to compare the results of present study with previous works. The level of LDL was not measured in the study as that parameter was not available in the autoanalyzer and determination of LDL by calculation gave inconsistent results. This was a limitation of the study. Ginkgo biloba was given to the animals for a short period of 2 weeks and the effect on the serum lipid profile was not studied a few months after stopping EGb 761 to see whether the effect was persistent. Other limitations of the study were the use of female wistar rats instead of rabbits as the model for hypercholesterolemia. Female rats were preferred because of availability and cost considerations. Hormonal variations during the estrous cycle may be a confounding factor. The possible mechanisms for the observed lipid lowering activity of EGb 761 were not investigated in the present study. Probucol, a hypolipidemic drug is a potent lipophilic antioxidant and the ability to inhibit atherosclerosis has been attributed to its antioxidant properties [ 18] . The flavonoids present in Ginkgo biloba may be responsible for its antioxidant as well as hypolipidemic action. The present study, however, has not investigated the mechanism of action of Ginkgo biloba. This should be explored further in future studies. Ginkgo biloba, according to reports from the literature has not been used clinically as a lipid lowering agent and we have not come across studies detailing the effect of EGb 761 on serum lipids. Previous studies investigating other effects of EGb 761 in rats and mice used doses ranging from 25 mg/kg to 100 mg/kg [19, 20] . In our study we had used three doses of EGb 761 for its effect on serum lipids. An estimation of liver enzymes at day 15 and day 30 may have been helpful in clarifying the biochemical changes which may have led to the lipid lowering action. However, this was not done in the present study. CONCLUSION The deleterious effects of high blood cholesterol and the beneficial effects of lowering blood cholesterol in reducing morbidity and mortality from cardiovascular diseases are well established. Non pharmacological measures like dietary restriction and exercise may help in lowering blood cholesterol levels. When such therapy fails, and in patients with abnormally high blood cholesterol levels, drug therapy is indicated [21] . The available drugs like statins, fibrates and nicotinic acid, though very effective, have a spectrum of adverse effects and are costly. The reason for interest in Ginkgo biloba was the low toxicity and the hope that it might be additive with other cholesterol lowering regimes. The results of this study showed significant lowering of serum cholesterol in Ginkgo biloba treated animals, almost comparable to that of lovastatin. But there was no significant effect on triglyceride and HDL levels. Further studies are required to establish the efficacy of the Ginkgo biloba extract (EGb 761) as a hypolipidemic drug. ACKNOWLEDGEMENTS EGb 761 was a gift sample from German Remedies, Mumbai, India. Lovastatin was a gift sample from Cipla pharmaceuticals, Mumbai, India. Their help is gratefully acknowledged. REFERENCES
Copyright © 2005 by Razi Institute for Drug Research (RIDR) The following images related to this document are available:Photo images[pt05002t2.jpg] [pt05002t1.jpg] [pt05002f1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}