 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
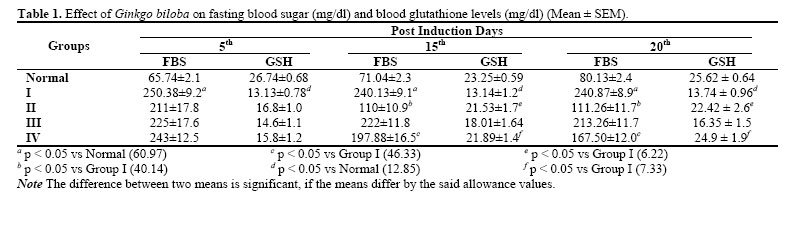
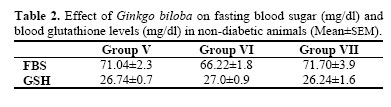
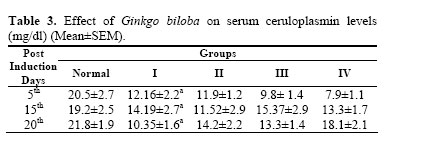
Iranian Journal of Pharmacology & Therapeutics, Vol. 4, No. 1, 2005, pp. 16-19 Evaluation of Antidiabetic Activity of Ginkgo Biloba in Streptozotocin Induced Diabetic RatsPINAKINI K SHANKAR, VASANTH KUMAR and NAMITA RAO Department of Pharmacology, Melaka Manipal Medical College (P.K.C.); Department of Pharmacology, Kasturba Medical College (V.K., N.R.) Manipal, India. Address correspondence to: Dr. Pinakini K Shankar , Assistant professor, Department of Pharmacology, Melaka Manipal Medical College, Manipal 576104, India. E-mail: pimochi@yahoo.co.in Received January 25, 2005; Code Number: pt05004 ABSTRACT The objective of the study was to evaluate the antidiabetic activity of Ginkgo biloba and to probe into its mechanism of action. Keywords: Ginkgo biloba, Antidiabetic, Antioxidant, Troglitazone Diabetics have significantly accelerated levels of oxidative stress and this contributes massively to most neurological, cardiovascular, retinal, renal diabetic complications [1] . A panoply of defenses against oxidative stress has evolved and operate at distinct levels. They are reduced generation of reactive oxygen species, enhancement of antioxidant enzymes like- Superoxide dismutase (SOD), catalase, glutathione peroxidase (GPX), and Glutathione Reductase (GSH) and repair systems at the level of DNA. Hyperglycemia significantly diminishes glutathione levels lowering defences against oxidative stress. N-acetyl cysteine a precursor of GSH inhibited the development of functional and structural abnormalities of peripheral nerves in experimental diabetes [ 2] . In contrast to these modalities, ceruloplasmin may contribute a mechanism to block the induction of oxidative injury through sequestration of tissue iron [ 3] . Though the role of oxidative stress in the development of diabetes mellitus and its vascular complications are extensively studied, there are very few therapeutic agents, which are targeted to this. Recently several thiazolidenediones such as troglitazone and pioglitazone have been developed as antidiabetic drugs. Of interest among these is troglitazone, which possess structural similarity to alpha tocopherol an established antioxidant [ 4] . Several studies have revealed the antioxidant properties of troglitazone, which complements the drugs hypoglycaemic, and hypolipidemic effects in diabetic patients [ 5] . Ginkgo biloba has been used in traditional Chinese medicine for 5000 years. Egb 761, its standardized preparation is used for a number conditions like cerebral insufficiency and peripheral vascular diseases. The Flavonoid glycosides in Egb 761 are responsible for its antioxidant activity and may prevent free radical dam age from occurring [ 6] . The therapeutic role of Ginkgo biloba extract on impairment of visual function and pathological histology of the optic nerve was studied in alloxan induced diabetic rats, which showed an increase in the amplitude of Visual Evoked potentials indicating axonal protection [ 7] . Egb 761 has also been found useful in the treatment of retinal impairment in diabetes [8] . A significant improvement of amplitude in the electroretinograms resulted from administering 100 mg/d of the extract for 2 months in alloxan induced diabetic rats [ 9] . Ginkgo biloba extract decreased the phagocytic activity of macrophages in alloxan induced diabetes, which indicate that it was effective in reducing lipid peroxidation in experimental diabetes [10]. Therefore, the present study was carried out to evaluate the antidiabetic activity of Ginkgo biloba in STZ induced diabetes and to probe into the mechanism of its antidiabetic property. MATERIALS AND METHODS The experiments were initiated after seeking approval from the institutional ethics committee. Animals Albino rats of wistar strain of either sex weighing, 150-200 gms bred in the central animal house Kasturba Medical College were used in the study. They were individually housed in polypropylene cages in well ventilated rooms, under hygienic conditions. Animals were given water ad libitum and fed with rat pellet feed (Hindustan Lever). Reagents Ginkgo biloba Egb761: Pure extract obtained from German remedies, Pvt. Ltd. Mumbai. Streptozotocin, 5.5’-Dithio-bis (2-nitrobenzoic acid) or Ellman’s reagent, Troglitazone and Glutathione (Sigma chemicals, U.S.A.). Glucose estimation kit was obtained from Ranbaxy Laboratories Ltd. Induction of Experimental Diabetes STZ solution of 10 mg/ ml was prepared in ice-cold citrate buffer 0.1 M, pH 4.5 kept in ice and was administered within 5 minutes at a dose of 50-mg/kg-body weight intraperitoneally. After 48 hours of STZ administration, rats with moderate diabetes having glycosuria and hyperglycaemia (i.e., with a blood glucose of 200-300 mg/dl) were taken for the experiment. Preparation of Drugs Ginkgo biloba was prepared as 1% gum acacia suspension. Troglitazone was prepared as 1% gum acacia suspension. Experimental Procedure Rats, weighing 150–200 g, fasted overnight were used for induction of diabetes.Rats was divided into two sets: Diabetic and non diabetic. In the diabetic set, 5 days after the induction of diabetes, animals were divided into 4 groups: Group I. received 1 % gum acacia and served as control. In the non diabetic group: Group V. Received 1% gum acacia and served as control. Rats were fasted overnight and blood was withdrawn from the retro orbital plexus on the fifth day of induction of diabetes and 15th and 20th day post induction (that is 10 and 15 days of drug treatment) for all groups and fasting blood sugar and ceruloplasmin level (in serum) and blood glutathione (in heparinised blood) were determined. Determination of Blood Glucose FBS was estimated by glucose oxidase peroxidase (Brief description may lee appropriate) method by using a glucose estimation kit from Ranbaxy laboratory Ltd. Determination of Blood Glutathione Blood glutathione was estimated by the method of Beutler et.al (Brief description may lee appropriate) [11] . Determination of Serum Ceruloplasmin Serum ceruloplasmin was estimated by using Diamine oxidase (Brief description may be appropriate) method [ 12] Statistical Analysis The results of the biochemical estimations were reported as Mean ± SEM. The total variation present in a data was analyzed by one-way analysis of variance (ANOVA). Differences among the means were analyzed by Scheffe’s test. For this an MS-Windows based SPSS computer package was used. RESULTSFasting Blood Sugar Levels (FBS) The FBS levels in STZ treated rats were significantly high (p < 0.05) when compared to the normal. The FBS values on the 15th day were 110 ± 10.9 mg/dl for Group II (troglitazone treated), 222 ± 11.8 mg/dl for Group III (Ginkgo biloba 50 mg/dl) and 197.88 ± 16.5 mg/dl for group IV (Ginkgo biloba 100mg/d) and on the 20th day were 111.25 ± 11.7 for Group II, 213.25 ±11.7 mg/dl for Group III and 167.5 ± 12.0 mg/dl for group IV (Table 1) . Troglitazone treated group (Group II) showed a significant decrease in the FBS levels (p < 0.05) that came near to the normal range on 10th and 15th day post treatment. Ginkgo biloba at the lower dose of 50 mg/kg (Group III) did not show a significant reduction in the blood sugar levels both on 10th and 15th day post treatment. However higher dose of Ginkgo biloba of 100 mg/kg (Group IV) showed a significant decrease in FBS (p < 0.05) on 10th and 15th day post treatment. However this reduction was not as much as that seen with standard drug troglitazone. Non-diabetic rats treated with Ginkgo biloba (Group VI & Group VII) at both the dose levels for 15 days did not exhibit any change in the FBS levels (Table 2) . Blood Glutathione LevelsThe GSH levels in normal rats were 26.74 ± 0.68 mg/dl. In STZ treated diabetic rats (Group I) the GSH levels decreased significantly (p < 0.05). Troglitazone treated rats (Group II) showed a significant increase (p < 0.05) in the GSH levels on both 10th and 15th post treatment days. Ginkgo biloba treated rats showed a significant increase (p < 0.05) in the blood GSH levels in the higher dose treated group (Group IV), whereas the low dose treated group (Group III) showed a mar ginal increase that was not significant (Table 1). Non-diabetic rats treated with Ginkgo biloba (Group VI & Group VII) at both the dose levels for 15 days did not exhibit any change in the GSH levels (Table 2) . Serum Ceruloplasmin LevelsThe serum ceruloplasmin level in normal rats was in a range of 18.2-24.8 mg/dl with a mean of 20.5 ± 2.7 mg/dl. In STZ treated diabetic rats the serum ceruloplasmin levels was 4.7-16.6 mg/dl with a mean of 10.35 ± 1.6 mg/dl, which was consistent till the 20th day. This showed a significant decrease (p < 0.001) when compared to the normal rats. However treatment with troglitazone and Ginkgo biloba at both doses did not alter the ceruloplasmin levels significantly (Table 3) . DISCUSSION In diabetes, oxidative stress is due to both an increased production of plasma free radical concentration and a sharp reduction of antioxidant defenses. GSH, being the most important biomolecule against chemically induced toxicity can participate in the elimination of reactive intermediates by reduction of hydro peroxides in the presence of Glutathione peroxidase. GSH also functions as free radical scavenger and in the repair of free radical caused biological damage [13]. The important mechanism implicated in the diabetogenic action of STZ is by increased generation of oxygen free radicals, which causes a decrease in plasma GSH concentration, and plasma GSH/GSSG ratio [ 14] . Hence, drugs that could prevent the generation of these oxygen free radicals or increase the free radical scavenging enzymes may be effective in STZ induced diabetes. In the present study the observed significant increase in blood glucose level in diabetic rats and a decrease in the level of blood GSH levels could be due to destruction of pancreatic ß cells by STZ reinforcing the view that STZ induces diabetes probably through the genera tion of oxygen free radicals [15] . The standard antidiabetic drug that was taken was troglitazone. It was shown that troglitazone could prevent the development of diabetes mellitus in mice injected with multiple low doses STZ, due to its antioxidant property [16]. Accordingly, our study also showed a significant decrease in FBS and an increase in blood GSH levels after treatment with troglitazone. Ginkgo biloba particularly the flavonoid component is known to be efficient in scavenging the highly reactive hydroxyl radical and superoxide anion and inhibits the lipid peroxidation by quenching the peroxyl radicals [ 17] . In contrast to a low dose of 50 mg/kg body weight, a higher dose of Ginkgo biloba (100 mg/kg body weight) has shown a significant reduction in fasting blood glucose levels which was comparable to that of troglitazone. Ginkgo biloba at higher doses has increased the antioxidant status in diabetic animals which is likely to have brought about its hypoglycaemic effect. Pancreas has a relatively weak defense system against oxidative stress, which can be externally strengthened. Antioxidants such as N-acetylcysteine and dietary antioxidants such as Vitamin C and E have shown to be beneficial in protecting the beta cells from glucose toxicity in diabetes [18] . Vitamin C and E, and lipoic acid, the natural antioxidants if supplemented have been shown to increase the levels of liver GSH in diabetic animals. GSH infusion has been shown to increase plasma GSH/GSSG ratio and potentiate the insu lin action in diabetic patients [ 14] . Thus, any drug that replenishes glutathione may be able to reverse the oxidative damage caused in diabetes mellitus and prevent the associated disorders. Ginkgo biloba, a known antioxidant, at higher dose probably strengthened the antioxidant status as evidenced by increase in the GSH levels than the lower dose and particularly so after 15 days of treatment. This may explain the dose dependent antidiabetic activity of Ginkgo biloba at higher dose level after 15 days of treatment. Ceruloplasmin forms a major part of the extracellular antioxidant defense. It also inhibits iron and copper dependent lipid peroxidation and also has a superoxide radical scavenging activity [ 19] . In our study diabetic rats showed a significant decrease in ceruloplasmin that may be so because of increased free radicals generated due to STZ. Neither Troglitazone and Ginkgo biloba treated diabetic rats did not show a significant improvement as seen with blood GSH levels indicating they probably do not have a significant role in metal ion mediated lipid peroxidation. Further study may be required to elucidate the action of Ginkgo biloba on ceruloplasmin, using higher doses and longer duration of treatment. In conclusion the present investigation showed that Ginkgo biloba by enhancing effect on cellular antioxidant defenses such as GSH has contributed to the protection against oxidative damage in STZ diabetes without significant effect on serum ceruloplasmin levels. REFERENCES
Copyright © 2005 by Razi Institute for Drug Research (RIDR) The following images related to this document are available:Photo images[pt05004t1.jpg] [pt05004t3.jpg] [pt05004t2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}