 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
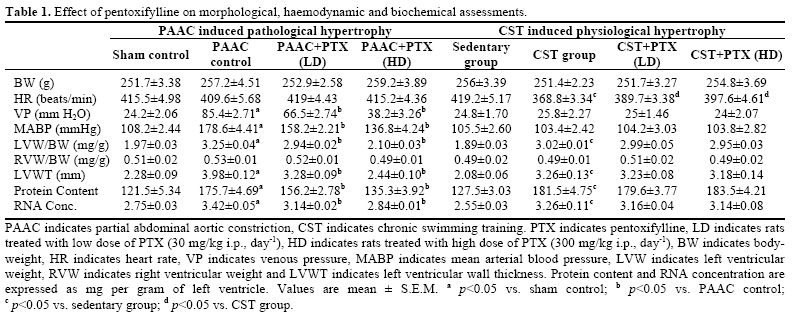
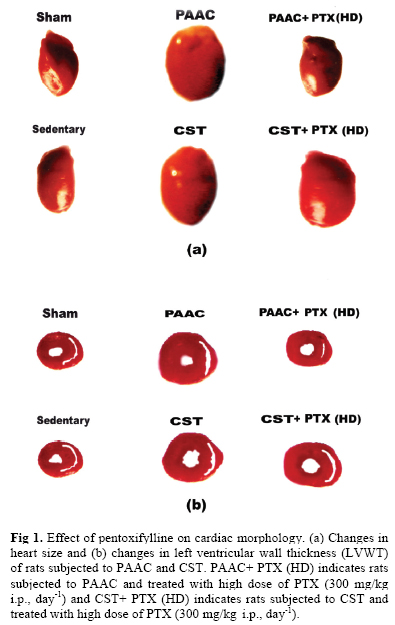
Iranian Journal of Pharmacology & Therapeutics, Vol. 4, No. 2, 2005, pp. 138-142 The Possible Role of TNF-α in Physiological and Pathophysiological Cardiac Hypertrophy in Rats PITCHAI BALAKUMAR and MANJEET SINGH Department of Pharmaceutical Sciences and Drug Research, Punjabi University, Patiala, India. Address correspondence to: Prof. Manjeet Singh, Dean of Medicine and Research, Department of Pharmaceutical Sciences and Drug Research,Punjabi University, Patiala, India. Phone: +91 (175) 3046304; Fax: +91 (175) 2283073. E-mail: pbala2002@rediffmail.com Received October 13, 2005; Revised February 28, 2006; Accepted March 1, 2006 Code Number: pt05029 ABSTRACT Pathological cardiac hypertrophy was produced by partial abdominal aortic constriction (PAAC) for 4 wk, while physiological cardiac hypertrophy was produced by chronic swimming training (CST) for 8 wk in rats. Pentoxifylline (30 mg/kg, 300 mg/kg i.p., day-1) treatment was started three days before PAAC and CST and it was continued for 4 wk in PAAC and 8 wk in CST experimental model. The left ventricular (LV) hypertrophy was assessed by measuring ratio of LV weight to body weight, LV wall thickness, LV protein content and LV RNA concentration. Further venous pressure (VP) and mean arterial blood pres-sure (MABP) were recorded. Moreover, DNA gel electrophoresis was employed to assess the myocardial cell death. The PAAC and CST were noted to increase the ratio of LV weight to body weight, LV wall thickness, LV protein content and LV RNA concentration. Further PAAC but not CST significantly in-creased VP, MABP and LV necrotic cell death. Pentoxifylline, a TNF-α inhibitor markedly attenuated PAAC induced increase in LV hypertrophy, VP, MABP and LV necrotic cell death; but it did not modulate CST induced LV hypertrophy. These results implicate TNF-α in PAAC induced cell death and pathological cardiac hypertrophy. However, TNF-α may not be involved in CST induced physiological cardiac hyper-trophy. Keywords: Aortic banding, Chronic swimming, Cardiac hypertrophy, Pentoxifylline, TNF-α Physiological adaptive eccentric hypertrophy is in-duced by exercise [ 1 , 2 ] and pathological concentric hypertrophy is associated with altered pattern of mal-adaptive cardiac gene expression [ 3 , 4 ]. Tumor necrosis factor-alpha (TNF-α), a proinflammatory cytokine has been implicated in pathogenesis of myocarditis, ischemic heart disease and cardiac dysfunction [ 5 - 7 ]. The prolonged exposures to high concentration of TNF-α produce cardiac dysfunction [ 8 ]. The persistent over expression of TNF-α has been suggested to be involved in cardiac hypertrophy and left ventricular dysfunction [ 9 - 11 ]. Moreover, the role of TNF-α in physiological cardiac hypertrophy is not yet clear. Pentoxifylline is reported to inhibit the production of TNF-α [ 11 - 15 ]. Hence, the present study has been designed to investi-gate the effect of pentoxifylline, an inhibitor of TNF-α in pathological and physiological cardiac hypertrophy. MATERIALS AND METHODS The experimental protocol used in the present study has been approved by institutional animal ethical committee. Young male wister albino rats weighing about 225-275 g were maintained on rat feed (Kisan Feeds Ltd., Chandigarh, India) and tap water ad libitum. They were housed in animal house and were exposed to 12-h light and 12-h dark cycle. Partial Abdominal Aortic Constriction (PAAC) Induced Pathological Cardiac Hypertrophy Pathological cardiac hypertrophy was produced using aortic banding [ 16 , 17 ]. Rats were anaesthetized with thiopentone sodium (35 mg/kg i.p.) and midline incision of 3-4 cm was made in abdomen to expose aorta between diaphragm and celiac artery. The 4-0 silk suture was placed around the middle of aorta and it was tightened along with a 0.7 mm diameter needle. The needle was withdrawn to leave the vessel partially constricted and midline incision was sutured in layers. Neo-sporin antibiotic powder (GlaxoSmithKline, Mumbai, India) was applied locally on the sutured wound. Rats were allowed to recover and were kept under observation for 4 wk. Sham operated animals were subjected to same surgical procedures except partial abdominal aortic constriction. Body weight was monitored weekly for 4 wk. Chronic Swimming Training (CST) Induced Physiological Cardiac Hypertrophy Physiological cardiac hypertrophy was produced using chronic swimming exercise programme [ 18 - 20 ]. The swimming apparatus was 150 cm in diameter and 45 cm in height. The water level was maintained at 30 cm. Rats were initially subjected to swimming for 30 min twice daily with increments of 10 min daily. The final duration of exercise was adjusted to 90 min; twice daily for 8 wk. Sedentary group animals were allowed to take rest without any disturbances. Body weight was monitored weekly for 8 wk. Morphological and Haemodynamic Assessments After 4 wk of PAAC and 8wk of CST, heart rate (beats/min) using ECG (BPL MK 801, Bangalore, India), jugular venous pressure (mmH2O) and carotid mean arterial blood pressure (mmHg) using pressure transducer (BIOPAC System, California, U.S.A) were recorded in anaesthetized rats. The left ventricle including interventricular septum and right ventricle weight were noted separately and expressed as mg per g of body weight. The left ventricle was divided into three equal slices and wall thickness (mm) of each slice was noted at eight different points using ocular micrometer. The mean value of all three slices were calculated and noted. Biochemical Assessments The left ventricle was stored at –80ºC in liquid nitrogen for quantitative estimation of biochemical parameters. The left ventricle was homogenized and protein content was determined spectrophotometrically at 750 nm by Lowry’s method [ 21 ] and expressed as mg/g of left ventricular weight. The RNA was extracted from homogenized left ventricular tissues using method of Chomczynski and Sacchi [ 22 ]. RNA concentration was estimated spectrophotometrically at 260 nm. One absorbancy unit at 260 nm in a 1 cm light path cuvette was assumed to be equal to 40 μg/mL of RNA. The purity of RNA was assessed by determining the ratio of absorbance at 260 and 280 nm and the ratio was more than 1.8. The DNA was extracted from homogenized left ventricular tissue using method of Ausubel et al [ 23 ]. The concentration of DNA was determined spectrophotometrically at 260 nm. The protein contamination of DNA was assessed by determining the ratio of absorbance at 260 nm and 280 nm, which was more than 1.75. DNA Gel Electrophoresis 12 μg of extracted DNA was added to equal volume of loading dye (40% sucrose, 0.1% bromophenol blue, 0.7% sodium dodecyl sulphate) and the mixture was loaded in the well. Electrophoresis was carried out using 1.8% agarose gel in 1 x TBE buffer (Tris HCl 89 mM, boric acid 89 mM, EDTA 2 mM) for 1.15 hr at 400 mA, 50V and 3W in submarine electrophoresis apparatus (Pharmacia Biotech, Freibury, Germany). Ethidium bromide (0.5μg/mL) was added to the gel for DNA detection. Experimental Design Rats were randomly divided into eight groups and each group comprised of six animals. Group 1 (Sham control, n=6), surgery was performed to expose the abdominal aorta but it was not constricted. Group 2 (PAAC control, n=6), abdominal aorta was exposed and partially constricted. Group 3 (Pentoxifylline 30 mg/kg i.p., day-1 treated, n=6), rats were subjected to partial abdominal aortic constriction and they were treated with low dose of pentoxifylline (30 mg/kg i.p., day-1) which was started 3 days before surgery and was continued for 4 wk after surgery. Group 4 (Pentoxifylline 300 mg/kg i.p., day-1 treated, n=6), rats were subjected to partial abdominal aortic constriction and they were treated with high dose of pentoxifylline (300 mg/kg i.p., day-1) as described in group 3. Group 5 (sedentary group, n=6), rats were allowed to rest without any disturbances. Group 6 (CST group, n=6), rats were subjected to chronic swimming exercise. Group 7 (Pentoxifylline 30 mg/kg i.p., day-1 treated, n=6), rats were subjected to chronic swimming exercise and they were treated with low dose of pentoxifylline (30 mg/kg i.p., day-1) 3 days before attaining 90 min swimming period and continued for 8 wk after attaining 90 min swimming period. Group 8 (Pentoxifylline 300 mg/kg i.p., day-1 treatment, n=6), rats were subjected to chronic swimming exercise and they were treated with high dose of pentoxifylline (300 mg/kg i.p., day-1) as described in group 7. Statistical Analysis Results were expressed as mean ± S.E.M. The data obtained from various groups were statistically analysed using one-way ANOVA followed by Tukey’s Multiple Range test. The p-value < 0.05 was considered to be statistically significant. Drugs and Chemicals Pentoxifylline was obtained from Aventis Pharma Limited, Mumbai, India. Proteinase K, sarcosyl, 2-mercaptoethanol and bovine serum albumin were purchased from Sigma-Aldrich, Louis, St. USA. Agarose and folin ciocalteu reagent were obtained from SRL, Mumbai, India. All other reagents used in this study were of analar grade. RESULTS Effect of Pentoxifylline on Morphological and Haemodynamic Assessments There was no significant change in body weight of rats subjected to sham surgery, 4 wk of partial abdominal aortic constriction (PAAC) and 8 wk of chronic swimming training (CST) with or without pentoxifylline treatment ( Table 1 ). PAAC produced no significant change in heart rate but it significantly increased venous pressure (VP) and mean arterial blood pressure (MABP). Pentoxifylline (30 mg/kg, 300 mg/kg i.p., day-1) treatment in a dose dependent manner signifi-cantly attenuated the increase in VP and MABP due to PAAC ( Table 1 ). PAAC increased the ratio of left ventricular weight to body weight (LVW/BW) (mg/g) and left ventricular wall thickness (LVWT), which were markedly attenuated in dose dependent manner by pentoxifylline (30 mg/kg, 300 mg/kg i.p., day-1) treatment ( Table 1 and Fig 1 ). CST did not produce any marked effect on VP and MABP. Moreover heart rate was markedly reduced as a result of CST and it was attenuated by pentoxifylline (30 mg/kg, 300 mg/kg i.p., day-1) treatment ( Table 1 ). The CST markedly increased ratio of left ventricular weight to body weight (LVW/BW) (mg/g) and left ventricular wall thickness (LVWT). But, pentoxifylline (30 mg/kg, 300 mg/kg i.p., day-1) treatment did not modulate increase in ratio of LVW to BW (mg/g) and LVWT due to CST ( Table 1 and Fig 1 ). There was no significant change in ratio of right ventricular weight to body weight (RVW/BW) (mg/g) of rats subjected to sham surgery, PAAC and CST with or without pentoxifylline treatment ( Table 1 ). Effect of Pentoxifylline on Biochemical Parameters PAAC and CST significantly increased protein content and RNA concentration in left ventricle. Pentoxifylline (30 mg/kg, 300 mg/kg i.p., day-1) treatment significantly attenuated PAAC induced increase in protein content and RNA concentration. In contrast to this, pentoxifylline (30 mg/kg, 300 mg/kg i.p., day-1) treatment did not modulate increase in protein content and RNA concentration in left ventricle due to CST ( Table 1 ). Effect of Pentoxifylline on Electrophoretic Pattern of DNA PAAC produced DNA smearing in agarose gel electrophoresis but CST did not produce any such effect. The DNA smearing is the marker of necrotic cell death. Pentoxifylline (30 mg/kg, 300 mg/kg i.p., day-1) significantly reduced PAAC induced DNA smearing ( Fig 2 ). DISCUSSION The partial abdominal aortic constriction (PAAC) [ 16 , 17 ] and chronic swimming training (CST) [ 18 - 20 ] have been employed in the present study to induce cardiac hypertrophy. Both the experimental models have increased ratio of left ventricular (LV) weight to body weight, LV wall thickness, LV protein content and LV RNA concentration which have been observed to increase in cardiac hypertrophy [ 24 - 27 ]. Pentoxifylline treatment markedly reduced PAAC induced cardiac hypertrophy measured in terms of above-mentioned parameters, but it failed to modulate CST induced cardiac hypertrophy. Pentoxifylline is reported to inhibit the formation of TNF-α [ 11 - 15 ]. The results of the present study implicate TNF-α in PAAC induced cardiac hypertrophy. On the other hand, TNF-α may not be involved in CST induced cardiac hypertrophy. DNA smearing is an index of necrotic cell death [ 28 ]. In contrast to the CST experimental model, PAAC induced cardiac hypertrophy has been noted to produce DNA smearing which suggest an increase in necrotic cell death in left ventricle. Moreover, pentoxifylline has been noted to attenuate PAAC induced increase in necrotic cell death perhaps due to inhibition of formation of TNF-α. The noted selective increase in venous pressure in PAAC model may be due to reduced left ventricular function as suggested by Philipp et al. [ 29 ]. The abdominal aortic constriction may be initially responsible to increase MABP, which has been observed to return to the normal value after about one and a half-hour of PAAC. However, MABP has been noted to increase gradually and attain peak level after 3-4 wk of PAAC. The marked increase in MABP in PAAC model may be due to pathological cardiac hypertrophy as reported recently [ 30 ]. The PAAC induced increase in venous pressure and MABP have been noted to be attenuated by pentoxifylline treatment. It suggests that TNF-α induced cardiac hypertrophy may be responsible to increase venous pressure and MABP. On the other hand, these haemodynamic changes have not been noted in CST induced cardiac hypertrophy. In conclusion, pentoxifylline induced inhibition of formation of TNF-α may be responsible for the attenuation of PAAC induced cell death and pathological cardiac hypertrophy. Moreover, TNF-α may not be involved in CST induced physiological cardiac hypertrophy. REFERENCES
Copyright © 2005 by Razi Institute for Drug Research (RIDR) The following images related to this document are available:Photo images[pt05029t1.jpg] [pt05029f1.jpg] [pt05029f2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}