 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pharmacology & Therapeutics, Vol. 5, No. 1, 2006, pp. 73-76 Research Article Comparison of Phosphate Lowering Properties of Calcium Acetate and Calcium Carbonate in Hemodialysis PatientsMassih Naghibi, Fatemeh Nazemian, Omid Rajabi, Maryam Hami Current Author Addresses Massih Naghibi, Nephrology ward of Imam Reza Hospital, Mashad University of Medical Sciences (MUMS), Mashad, Iran, Associate Professor of Nephrology; E-mail: mnaghibi_md@yahoo.com Received September 2, 2005; Revised May 29, 2006; Accepted June 5, 2006 Code Number: pt06001 ABSTRACT Hyperphosphatemia has an important role in the development of secondary hyperparathyroidism and bone disease in patients with end-stage renal disease (ESRD). The most effective method of phosphate elimination lies with phosphate binders, the agent that more commonly used, calcium carbonate, is not an ideal binding agent. In this regard, calcium acetate has been reported to have more or at least a similar phosphate binding efficacy and less pronounced hypercalcemic effect. However, this subject is still a matter of controversy. This study was designed to compare the efficiency of these salts. Preparation of calcium acetate and comparison of the phosphate binding power and hypercalcemic effect of calcium acetate with that of calcium carbonate in hemodialysis patients. Thirty stable ESRD patients undergoing regular hemodialysis for mean 4.23 years (SD 3.63) were studied. Half of the patients were started on calcium acetate for a month. Then, after two weeks wash out period, they received calcium carbonate for a month. The others followed an inverse protocol. 24 patients completed the study. A significant decrease in plasma phosphate levels was only observed after treatment with calcium acetate [6.65 mg/dL (SD 1.38) vs. 5.83 mg/dL (SD 1.55) p < 0.05]. Calcium acetate may be a better choice in handling of hyperphophatemia in ESRD patients and when calcium acetate is used, control of hyperphophatemia can be better achieved with a lower risk of hypercalcemia. Keywords: Calcium acetate, Hemodialysis, Hypercalcemia, Hyperphosphatemia Hyperphosphatemia has an important role in the development of secondary hyperparathyroidism and bone disease in patients with end stage renal disease [1, 2]. Increased calcium x phosphate product has been linked to increased mortality and a high burden of cardiac calcification [3, 4]. Then hyperphosphatemia is a silent killer of patients with renal failure [5]. Reports indicate that patients found with phosphate levels greater than 6.5 mg/dL have a 27% higher mortality risk than patient with levels ranging between 2.5 to 6.5 mg/dL. Unfortunately, it is often difficult to reduce phosphorous intake without also reducing intake of essential proteins, thereby limiting the effectiveness of dietary restriction. The most effective method of phosphate elimination lies with phosphate binders [6]. The most commonly used, calcium carbonate, is not an ideal binding agent. It is reported that the phosphate binding power of calcium acetate is about twice the phosphate binding power of calcium carbonate [7]. This may be due to the fact that calcium carbonate can be dissolved only in an environment with an acid pH and many patients with advanced renal failure have achloridria or are taking H2 blockers [6-8]. Absorption of calcium from calcium acetate in GI tract is 40% while fasting and less than 30% for postmeal condition.which is less than the absorption from calcium carbonate. Therefore, it has less hypercalcemic effect too. However, this subject is still a matter of controversy [9]. This study is designed to compare the efficiency of these salts in phosphate binding power. Materials and Methods Design and Tablet Formulation At first determination of physicochemical properties of calcium acetate as powder (amount of water as hydrated, compressibility, amount of Ca2+) was done. Then, granules were prepared by wet granulation method. Size distribution, friability, flow ability, compressibility and density (tap and bulk) of granules were determined. The results of above determinations were used for selection of the best granules (the best formulas) for tablet preparation. Clinical StudyThirty stable ESRD patients undergoing regular hemodialysis in Imam Reza hospital dialysis ward for mean 4.23 years (SD 3.63) entered to study. Parathyroidectomized patients were not included. Dialysis was performed three times a week utilizing a polysulfone R4 and R5 membrane with a surface area of between 0.7 m2 and 1 m2, dialysis sessions were accomplished using blood flow of 300-400 m2/min and acetate buffered dialysate [ca]=2.5meq/l at 500cc/min dialysate flow rate. Patients used calcium carbonate and/or 1,25(OH)2D3 in variable doses, which was withdrawn for a period of two weeks before the beginning of study. All other types of medication, such as antihypertensive agents, B complex, folic acid and erythropoietin were maintained. The study was conducted in a cross over, randomized manner. Half of the patients were initiated on 3g/day calcium carbonate (1200 mg Ca2+) for 4 weeks followed by a wash out period of two weeks. After this period they received 2.7 g/day of calcium acetate (676 mg Ca2+) for another 4 weeks. The remaining patients followed a similar protocol, but were initially given calcium acetate and then calcium carbonate. They were all instructed to take the medication after meals in such a way that the whole daily dose would be divided into two or three doses according to the dietary habit of the patients. Clinical interviews were conducted three times a week to monitor for adverse effects. Serum urea, calcium, phosphate, blood gas analysis, hematocrit and KT/V determinations were performed before and after each treatment. The trial was performed in accordance with the Declaration of Helsinki and approved by the ethics committee at Mashad University of Medical Sciences. Written informed consents were obtained before entering into the study.
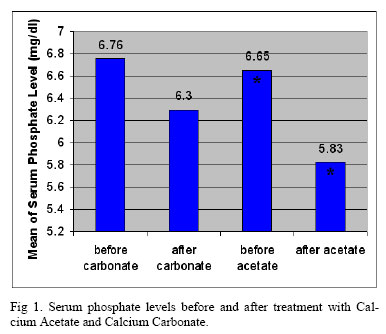
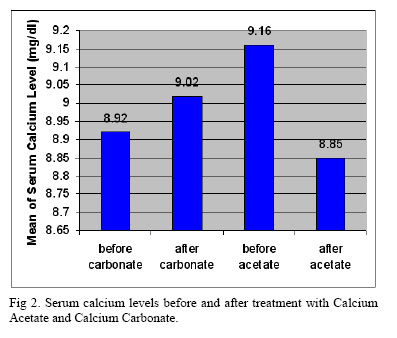
Statistical Method Data was expressed as mean and standard deviation (SD) or median and range, depending upon the pattern of distribution. Frequencies were evaluated by the chi-squared test, T-test. Differences in percent variation of calcium and phosphorous between salts, and ratios of these percent variations, were evaluated by the nonparametric sign rank test, Wilcoxon signed ranks test and Npar test. Values of p less than 0.05 were considered significant. ResultsThirty subjects entered the study and twenty- four were included in the data analysis. The general features of the patients are described in the Table 1. Four patients who had kidney transplantation, one patient who had GI intolerance and one patient who had increased muscle cramp, were excluded from the study. Table 2 summarizes the laboratory findings from pre and post treatment with calcium acetate and calcium carbonate. None of the preparations significantly altered the values of blood pH, bicarbonate and HCT, ALP, Ca, PTH. A significant decrease in phosphate level was only observed after treatment with calcium acetate (5.83 mg/dL (SD 1.55) vs. 6.30 mg/dL (SD 1.74), p < 0.05) (Fig 1). The post-treatment plasma calcium levels between the two compounds, however, did not differ statistically (Fig 2). There were no significant changes in KT/V throughout the study. Analysis suggests that more phosphate be bound by each equivalent of calcium acetate in comparison to calcium carbonate. DiscussionHyperphosphatemia has been implicated in different manners in the genesis of parathyroid hyperfunction as directly on parathyroid gland and indirectly by decreasing ionized calcium and 1,25(OH)2D3. It stimulates hyperplasia of the parathyroid glands and osteitis fibrous cystica (high turn over bone disease) [10]. It can also contribute to precipitation of metastatic vascular and nonvascular calcification such as coronary plaques, cardiac valves and myocardial tissue calcification as well as diffuse myocardial fibrosis [4]. Also it’s accepted in other studies that cardiovascular disease is the most frequent cause of death in ESRD patients [10].
Control of Hyperphosphatemia has been linked to decrease mortality [8-11]. These reinforce all these reasons in favor of there being an adequate control of serum phosphate levels in uremia [12]. About 40% to 80%of phosphate in the foods is absorbed in bowel of patients with renal failure, then using a phosphate binder is an effective method to control of hyperphosphatemia [6]. In present study, calcium carbonate and calcium acetate were compared regarding their phosphate binding properties and hypercalcemic effects and tolerance. The protocol was designed in such a way that comparable doses (in grams) of each salt were given during each phase of the study. In this content, the daily amount of calcium prescribed was always lower with calcium acetate. The study dropout ratio for each compound was low and without statistical difference statistically. Tolerance and side effects were also comparable, although upper GI intolerance and muscle cramp were seen in two patients in acetate group. A detailed examination of the different reasons for exclusion did not show statistically significant differences. Therefore, the acceptance of the compounds was similar. Neither acetate nor carbonate induced significant changes in blood pH, Hct, KT/V and bicarbonate and ALP and PTH and calcium. Relevant alteration was restricted to phosphate plasma levels. A significant decrease in plasma phosphate levels was only observed after treatment with calcium acetate [6.65 mg/dL (SD1.38) vs. 5.83mg/dL (SD1.55) p < 0.05], which is consistant with studies reporting a less hypercalcemic effect for calcium acetate [12]. A statistically nonsignificant rise in calcium level [8.85mg/dL (SD 0.72) vs. 9.02 mg/dL (SD0.88)] was only found with carbonate. This finding could simply be accounted for by the lower amount of elemental calcium given during calcium acetate treatment [6]. In one study, about skeletal effects of calcium acetate, the result was bone mineral density increase in lumbar vertebrae. It may be because of better control of calcium acetate on parathyroid hormone. The duration of study was 24 weeks [13, 14]. As in another study, they found that serum phosphate level was significantly lower after treatment with acetate than with carbonate as was the Ca x P product and PTH (the duration of study was 6 weeks) [15]. However in our study, there wasn’t a significant difference in PTH between two groups, it may be because shorter period of this study and for detection of effects of calcium acetate on bone density we need more time. Recently, it is reported that calcium acetate controls serum phosphate and calcium x phosphate product more effectively than sevelamer hydrochloride. Cost benefit analysis indicates that in the absence of hypercalcemia, calcium acetate should remain the treatment of choice for hyperphosphatemia in hemodialysis patients [2]. AcknowledgementThis study was supported by a grant from Mashad University of Medical Sciences. References
Copyright © 2005 by Razi Institute for Drug Research (RIDR) The following images related to this document are available:Photo images[pt06012f1.jpg] [pt06012f2.jpg] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||
{kind=link}
{kind=link}