 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pharmacology & Therapeutics, Vol. 5, No. 2, 2006, pp. 131-133 Research Article Intranasal Sufentanil for Postoperative Pain Control in Lower Abdominal Pediatric SurgeryFarhad Heshmati, Heidar Noroozinia, Rahman Abbasivash, Alireza Mahoori and Helen Gharaee Current
Author
Addresses: Farhad
Heshmati,
MD.
Associate
professor
of
anesthesiology,
Urmia
University
of
Medical
Sciences,
Department
of
Anesthesiology,
Urmia
University
of
Medical
Sciences,
Urmia,
Iran.Fax:
+98
(441)
3469935
E-mail: f_heshmati@umsu.ac.ir (Corresponding
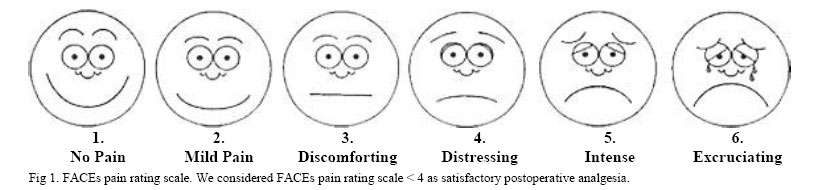
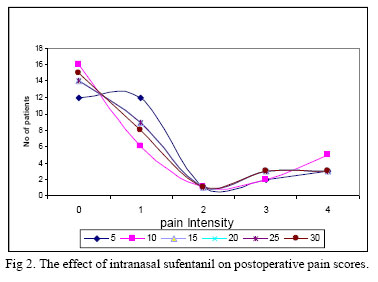
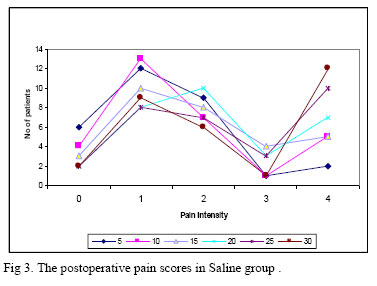
author). Received May 24, 2006; Revised September 28, 2006; Accepted October 3, 2006 Code Number: pt06022 ABSTRACT The most important role in postoperative pain management is still played by opioid administration through various modes. For the last few years, there has been an intensive search for alternative mode of opioid administration in pain management. The intranasal modes of opioid administration seems to be an attractive alternative. Sixty boys (aged 0.5-6 yr); ASA (American Society of Anesthesiologists) physical status I, who were candidates for lower abdominal surgery, were included in this prospective randomized, controlled study. Five minutes before extubation, patients were randomized to two groups and allocated to receive intranasal sufentanil (0.7 µg/kg) or normal saline, using a double-blinded study design. Satisfactory analgesia was achieved with intranasal sufentanil. It was effective after 10 minutes with the least pain scores (pain score 2.3±0.4 vs. 4.1±0.5) (p = 0.001). Pain scores in 15, 20 and 25 minutes were similar in sufentanil group. None of patients had bradycardia, hypotension or SpO2 (arterial O2 saturation) <95%. High bioavailability of sufentanil after intranasal administration due to direct entrance of the drug into the systemic circulation and avoidance of the hepatic first- pass effect makes sufentanil an opioid with rapid onset and limited duration. As it has minimal side effects, sufentanil is one of the best choices for postoperative pain control in children. We used 0.7 µg/kg of intranasal sufentanil and found satisfactory analgesia accompanied with least side effects. Keywords: Analgesia, Intranasal, Sufentanil, Pediatric, Postoperative pain It is now accepted that pain should be anticipated, safely and effectively controlled in all children, whatever their age, maturity or severity of illness. Unfortunately the postoperative pain in pediatric patient is not adequately managed [1]. The most important role in postoperative pain management is still played by opioids administered through various modes. In the last few years, there has been an intensive search for alternative mode of opioid administration in pain management. The intranasal mode of opioid administration seems to bean attractive alternative, especially in patients who have not intravenous access. Supported by extensive research into novel form of drug delivery, nasal administration of medications is emerging as a promising method of delivering drug with several advantages [2]. Pharmacokinetic studies have demonstrated a high bioavailability (71%, 65% and 78%) and a rapid rise in plasma concentrations follow intranasal fentanyl, alfentanil and sufentanil. Sufentanil is the most extensively used for sedation [3]. The elimination half life of intravenous sufentanil is 15-20 minutes [4]. Intranasal administration induces no clinically significant change in vital signs, whereas after intravenous sufentanil, a clinically significant decrease in PaO2 (arterial partial pressure of oxygen) is seen at 5 min [5]. MethodsAfter approval by University Research Committee and obtaining parental consent, sixty normal healthy boys, aged 0.5-6 yr, scheduled to lower abdominal surgery (such as, herniorrhaphy, orchiopexy, hydrocellectomy, urethroplasty) undergoing general anesthesia enrolled in this prospective double blinded study. Exclusion criteria included emergency operations and upper respiratory tract infection. All patients received fentanyl 1mg/kg and atropine 10 µg/kg before induction of anesthesia. Induction of anesthesia accomplished with thiopenthal Na 6 mg/kg and atracurium 0.6 mg/kg (for facilitation of tracheal intubation). Anesthesia was maintained by administration of halothane and N2O in 50% O2. Patients randomized (according to table of randomized numbers) in two groups, group 1 (n=30) received intranasal normal saline (N/S) and group 2 (n=30) received intranasal sufentanil (0.7 µg/kg), 5 min before extubation. Heart rate, blood pressure, respiratory rate, arterial O2 saturation (PaO2), vomiting, pain and sedation scores were recorded by a nurse who was not informed of the content of administrated solutions. Pain was measured according to FACEs pain rating scale (Fig 1) and sedation was measured according to Ramsay Sedation Scale at arrival and every 5 min until 30 min in recovery room. We considered FACEs pain rating scale < 4 as satisfactory postoperative analgesia and Ramsay Sedation Scale ³4 as over sedation. Data Analysis To analyze differences between two groups Log linear models was used. Fisher-Exact test was considered for nominal data using SPSS software. Statistically differences between two groups of patients was considered at p<0.05. ResultsThere was no difference between the groups, with respect to age, weight, duration of surgery and anesthesia. Pain scores were significantly reduced in sufentanil group vs. normal saline group (pain score 2.3±0.4 vs. 4.1±0.5) (p=0.001). Sufentanil was effective after 10 minutes with the least pain scores (Fig 2, Fig 3). Pain scores in 15, 20 and 25 minutes were similar in sufentanil group. Patients did not have bradycardia, hypotension or SpO2 <95%. Two patients in sufentanil group had nausea, which in one of them occurred immediately after instillation of drug. This problem might be not related to sufentanil. It seems the cause of nausea in this patient was related to awake extubation. Four patients in sufentanil group and two patients in normal saline group had over sedation. But none of them SpO2 <95% or loss of protective reflexes. DiscussionOur results show that intranasal sufentanil is quite effective in relieving pain in pediatric patients. Most patients experienced significant pain relief after 10 min. As the lipid solubility of sufentanil is two times more than that of fentanyl [6]. Helmers et al. also suggested a higher
bioavailability of sufentanil after intranasal administration. This higher
bioavailability is due to direct entrance of the drug into the systemic circulation
and avoidance of the hepatic first-pass effect. They compared intranasal and
intravenous absorption and sedation preoperatively. Preoperative sedation of
rapid onset and limited duration was seen in both groups. At 10 min, all
patients in the intravenous group were sedated versus only two in the
intranasal group (p <0.01).
From
30
min,
plasma
concentrations
were
virtually
identical
for
the
two
routes
of
administration.
Intranasal
administratiom
induced
no
clinically
significant
changes
in
vital
signs,
whereas
after
intravenous
sufentanil,
caused
a
clinically
significant
decrease
in
PaO2 at 5
min [5]. Intranasal fentanyl as an opioid is associated
with diminished postoperative agitation without increasing vomiting, hypoxemia,
or discharge time, when used during anesthesia for myringotomy [7]. Safety and efficacy of intranasal fentanyl in
reducing acute pain of children in the emergency department was reported.
Significant reduction in pain intensity (10 min after administration) with
duration of analgesia for 30 min was seen [8].
Intranasal midazolam and sufentanil as premedication were compared in 60
pediatric outpatients. Approximately 15-20 min after drug administration, most
patients in both groups could be comfortably separated from their parents. The
sufentanil group appeared to be more sedated and more cooperative during induction
of anesthesia. Vital signs and SpO2 did not change significantly
with either medication before or after surgery. Sufentanil was associated with
more nausea and vomiting than midazolam (34% vs. 6%, p<0.02).
In
conclusion,
both
intranasal
midazolam
and
sufentanil
provide
rapid,
safe,
and
effective
sedation
in
small
children.
Sufentanil
provided
somewhat
better
conditions
for
induction
and
emergence.
Patients
in
the
midazolam
group
were
discharged
approximately
40
minutes
earlier
[9].
Response
to
sufentanil
was
more
variable
in
patients
groups
[10,
11].
Sufentanil 1.5 µg/kg IV ten minutes before the end of surgery had very satisfactory results for postoperative pain relief [12]. Using intranasal sufentanil for break through and incident cancer – associated pain, has been reported with no adverse effects such as vomiting or respiratory depression [13]. In a study intranasal sufentanil (1.5, 3.0, or 4.5 µg /kg) was compared by placebo (normal saline, 0.03 ml/kg). Induction of anesthesia was completed with 5% halothane and O2 via facemask. After tracheal intubation, anesthesia was maintained with N2O (60-70%) and halothane, as clinically indicated. A blinded observer remained with the child from prior to drug administration until discharge from the recovery room. Patients given sufentanil were more likely to separate willingly from their parents and be judged as calm at or before 10 min compared to those given saline. Sufentanil, 4.5 µg/kg, had a higher incidence of vomiting in the recovery room and during the first postoperative day [14]. Intranasal sufentanil (10 or 20 µg) has been successfully used for preoperative sedation in adult patients [15]. We chose sufentanil because of its high bioavailability, rapid onset, short duration and minimal side effects. According to these studies, we used 0.7 µg/kg sufentanil and found it very effective and safe. Side effects such as nausea and over sedation were in acceptable range. We recommend using it as postoperative analgesic in operating room and post anesthesia care unit (PACU), as premedication or even as triage nurse- initiated administration in the emergency department. References
Copyright © 2006 by Razi Institute for Drug Research (RIDR) The following images related to this document are available:Photo images[pt06022f3.jpg] [pt06022f2.jpg] [pt06022f1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}