 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pharmacology & Therapeutics, Vol. 5, No. 2, 2006, pp. 135-139 Research Article Renoprotection by Telmisartan versus Benazepril in Streptozotocin Induced Diabetic NephropathyJanardhan singh, salil budhiraja, harbans lal, brij rani arora Current
Author
Addresses: Janardhan
Singh,
Associate
Professor,
Department
of
Pharmacology,
PGIMS,
Rohtak-124001
(Haryana-India). Received May 11, 2006; Revised October 4, 2006; Accepted October 10, 2006 Code Number: pt06023 ABSTRACT Diabetic nephropathy (DN) is one of the major causes of end stage renal disease. Angiotensin converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARB) are preferred for delaying progression of DN. This study compared the preventive renal effects of telmisartan (10 mg/kg, p.o.), an ARB, that completely blocks angiotensin action, and benazepril (5 mg/kg, p.o.), an ACE inhibitor, which is a partial blocker of angiotensin II production, in an animal model of diabetic nephropathy. DN was induced by streptozotocin (50 mg/kg, i.p.) single injection in male albino rats. Biochemical parameters (creatinine clearance, urinary protein and blood urea) were significantly (p<0.01) altered in diabetic rats after 4 weeks. Telmisartan (10 mg/kg, p.o.) and benazepril (5 mg/kg, p.o.) treatment significantly (p<0.01) reduced elevated levels of blood urea and urinary protein in diabetic rats. After 8 weeks of diabetes there was significant difference in reduction of blood urea in between telmisartan and benazeril group. Difference between telmisartan and benazepril for reduction in proteinuria was not singnificant. Difference between telmisartan and benazepril for creatinine clearance improvement was also not significant (p>0.05). Histology revealed beneficial effects produced by both drugs. This study demonstrates telmisartan is equally renoprotective as benazepril. Keywords: Diabetic nephropathy, STZ, Telmisartan, Benazepril Diabetic nephropathy (DN) is one of the most serious problems in nephrology, as 40% of the cases of end stage renal disease (ESRD) are due to this entity. Angiotensin ІІ plays an important role in mediating proteinuria by various mechanisms including hyperfiltration, opening of nonselective pores in the ultrafiltration barrier, modifying the composition of glomerular basement membrane and reducing nephrin expression on podocytes. Agents blocking the renin angiotensin system (RAS), angiotensin converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARB), are preferred for preventing albuminuria and delaying progression of DN [1]. Currently, ACE inhibitors are the first line drugs and ARBs are used in those patients who cannot not tolerate ACE inhibitors. There is controversy regarding preferable method for RAS blockade in diabetes, which started after the discovery of ARB. ARBs produce complete blockade of angiotensin ІІ effects while ACE inhibitors partially block the generation of angiotensin ІІ. Crook and Penumalee [2] suggested that there was no significant difference between ACE inhibitors and ARBs with regard to renal outcomes in DN. Abott and Bakris [3] suggested that the greatest benefit for slowing progression of renal disease in DN now belongs to ARB. Hsueh also suggested that effects of ACE inhibitor in slowing the progression to ESRD which have not been clearly demonstrated in type 2 DN [4]. Therefore the present study was undertaken to evaluate the role of an ARB (Telmisartan) and an ACE inhibitor (Benazepril) in streptozotocin (STZ) induced diabetic nephropathy. Material and Methods Animal Model Male albino rats (HAU, Hisar strain) 8-10 weeks old, weighing (230-280 g), were used. Rats were fed with standard food pellets and water ad libitum, housed in cages under 12/12 dark/light cycle. The experimental protocol met the national guidelines on the proper care and use of animals in the laboratory research and an institutional animal ethics committee approved the study. Study GroupsFollowing the induction of diabetes, the animals were randomly allocated into four groups (n =10) and treated for 16 weeks as follows:
Induction of Diabetes Diabetes was induced by single injection of streptozotocin (STZ) at a dose of 50 mg/kg, i.p. dissolved in 0.01M citrate buffer (pH 4.5) after 16 h fasting. 72h after STZ injection diabetes was confirmed in rats showing blood sugar level greater than 250 mg/dL. Animals with blood glucose levels greater than 250 mg/dL were considered for further study. Blood samples were collected. 72 hours after STZ administration, and thereafter every 4 weeks from orbital plexus by pricking a needle under ketamine anaesthesia. Glucose-Oxidase assay method [5] was used to determine the blood glucose. Biochemical ParametersNephropathy was evaluated by estimating blood urea [6] and urinary proteins [7]. Further creatinine clearance was also determined as a measure of glomerular filtration rate (GFR). Creatinine clearance was assessed from the urinary [8] and serum creatinine [8] and expressed as mL/min/kg body weight. Blood urea was estimated by diacetyl monooxime method. Serum and urinary creatinine were measured by alkaline picrate method (Jaffe’s method). Urinary protein was measured by precipitation with trichloroacetic acid and the precipitate was dissolved in 1N NaOH and quantitated by Biuret method.
Histological Assessment of Kidney Injury Light microscopy- At 16 weeks, portions of kidney were obtained and fixed in 10% buffered formalin. Staining procedures were performed by standard techniques in our laboratory. [9] Paraffin sections were cut at 3 μm and stained with hematoxylin and eosin, periodic acid-Schiff (PAS) and silver methanamine. All glomeruli in randomly selected sections were examined under high power fields for evidence of sclerosis. Histometrical measurements- The degree of glomerulosclerosis was evaluated by semiquantitative method [10]. A total of 50 glomeruli from each specimen were graded according to severity of the glomerular damage. The degree of sclerosis in each glomerulus was subjectively graded on a scale of 0 to 4: Grade 0- no change; Grade 1- slight glomerular damage, mesangial matrix and/ or hyalinosis with sclerotic area less than or equal to ¼ of glomerulus; Grade 2- sclerosis of ¼ to ½ total glomerular area; Grade 3- sclerosis of more than ½ the glomerulus but not global and grade 4- global sclerosis. Mean score of glomerulosclerosis was calculated in each study group and compared. Statistical AnalysisAll data are shown as mean±SEM unless otherwise specified. Results were analyzed by analysis of variance (F-test). Significance between the groups was estimated using Student’s t-test. A P value of less than 0.05 was considered as statistically significant.
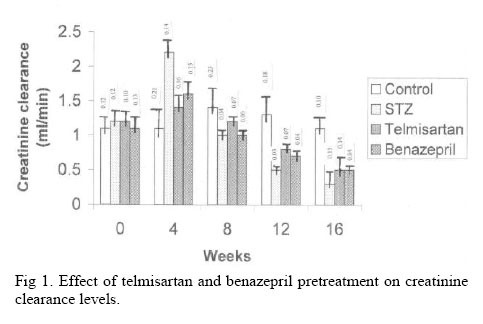
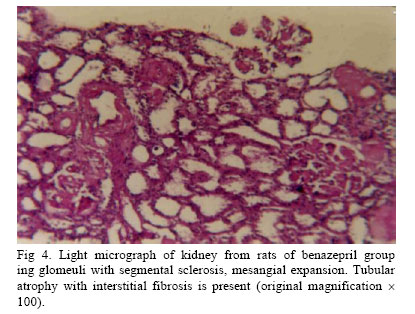
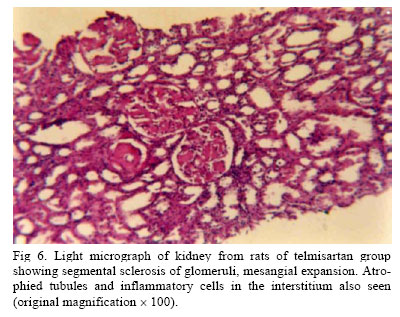
Results Metabolic parameters. Group 1 (control) animals showed a gradual increase in body weight while group 2 (diabetic control) was associated with marked and gradual reduction in body weight. In group 3 and 4 animals treated with telmisartan and benazepril respectively, the decrease in body weight was suppressed.
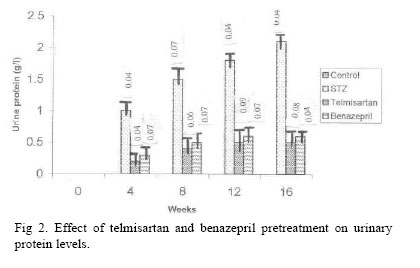
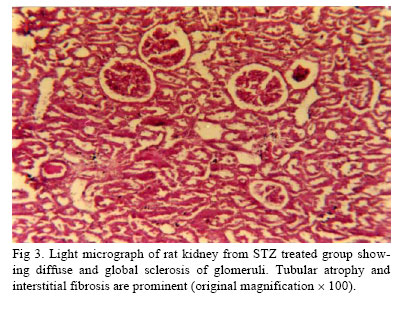
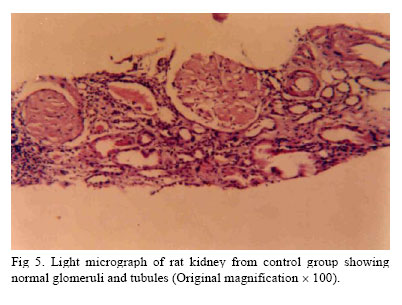
In STZ diabetic rats there was a significant (p<0.001) and sustained increase in blood glucose levels. Telmisartan and benazepril pretreatment alter blood glucose levels significantly (p<0.05) in STZ diabetic rats after 12 weeks. (Table 1). Biochemical parameters. Creatinine clearance was taken as a parameter to assess GFR. In the early weeks of diabetes, there was a significant (p<0.05) increase in creatinine clearance that gradually decreased in later weeks. Group 3 and 4 had decreased rise in GFR in early weeks as compared to diabetic rats but less decline in GFR was observed during later weeks as compared to group 2 rats. However, the beneficial effects of these drugs on GFR were not statistical significant (p>0.05) (Fig 1) and the difference between telmisartan and benazepril group was not statistically significant. Urinary protein excretion was not observed in any rat from control group. In the control group there was no excretion of protein in urine. However, there was a significant (p<0.001) and sustained increase in urinary protein excretion after 4 weeks of STZ. Telmisartan and benazepril pretreatment significantly (p<0.001) retarded the increase in proteinuria compared with the untreated diabetic group (Fig 2). There was no significant difference in reduction of proteinuria between telmisartan and benazepril pretreatment group. There was a significant (p<0.001) increase in blood urea in STZ diabetic animals as compared to control group. Telmisartan and benazepril pretreatment significantly (p<0.001) reduced the elevated levels of blood urea in diabetic rats (Table 2). However, when compared with benazepril pretreated group, reduction in blood urea level was significantly (p<0.05) higher in telmisartan group after 8 weeks. Histology. Light microscopic findings-Histology of control rat kidney showed normal glomeruli, renal tubules and blood vessels. (Fig 3) After 16 weeks of STZ administration severe and gross changes were observed in kidneys. Diabetic rats had increased glomerulosclerosis and tubulointerstitial injury when compared to control rats. Most of the glomeruli showed diffuse sclerosis while remaining glomeruli also showed segmental sclerosis with basement membrane thickening and increased mesangial matrix expansion with wide spread interstitial fibrosis. Most of the tubules were atrophied (Fig 5). Increased glomerulosclerosis and tubulointerstitial injury in diabetic rats were reduced by telmisartan and benazepril pretreatment. (Fig 4, Fig 6) Histometrical studies. Mean glomerulosclerosis score was significantly increased in the diabetic rats compared to controls. The score was 3.2±0.42 in diabetic rats. Telmisartan and benazepril prevented the increase in mean glomerulosclerosis score to (1.8±0.42) and (2.0±0.48) respectively. DiscussionThe results of the present study demonstrate that both telmisartan and benazepril attenuate the development of proteinuria, prevent kidney structural injury and elevation of blood urea. This study also shows that telmisartan reduced elevated blood urea level more effectively as compared to benazepril whereas preventive effect on proteinuria and GFR were comparable. These findings suggest that telmisartan may be used as a first line drug in preventing pathological injury in the diabetic kidney. In diabetic rats glomerular angiotensin II levels are increased due to increase in angiotensinogen [11]. ACE inhibitors do not fully block production of angiotensin II from angiotensinogen because of up regulation of some non-ACE pathways (chymase enzyme) in kidneys [12]. Angiotensin II is known to produce deleterious effects on kidney by affecting the blood pressure and renal haemodynamics, production of growth promoting and profibrotic factors, renal tubular and glomerular hypertrophy and oxidative stress in kidney [13]. Therefore, blockade of angiotensin II is very important factor for halting the progress of DN. It is well supported by the fact that although ACE inhibitors afford a degree of renal protection, DN continues to progress relentlessly albeit at a slower rate [14]. There is also possibility of increased fibrosis in vascular smooth muscle cells of kidney via modulating TGF-ß, MAPK pathways due to elevated blood levels of bradykinin produced by ACE inhibitors [15]. This may be one of the important factors responsible for decreased effectiveness of ACE inhibitor on long term use. RAS blockers have preventive action on DN, independent of its decrease in blood pressure effects but ARBs more effectively block biological effects of Ang II. Presently ACE inhibitors are first choice drugs for diabetic nephropathy. It is suggested from our study that ARB are equieffective as ACE inhibitor and can be used as a first line drug to retard the progression of DN and with the use of ARB we can prevent the side effects of ACE inhibitor. However, more studies are required to confirm it. References
Copyright © 2006 by Razi Institute for Drug Research (RIDR) The following images related to this document are available:Photo images[pt06023f6.jpg] [pt06023f3.jpg] [pt06023f1.jpg] [pt06023f4.jpg] [pt06023f5.jpg] [pt06023f2.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}