 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
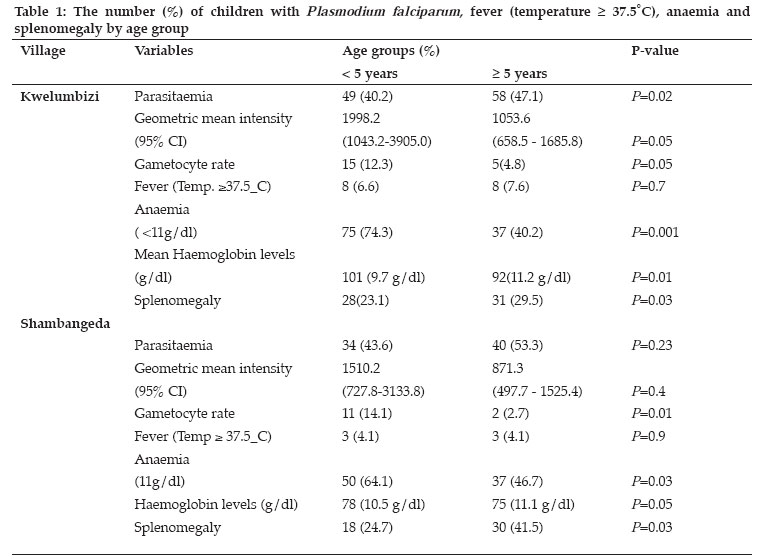
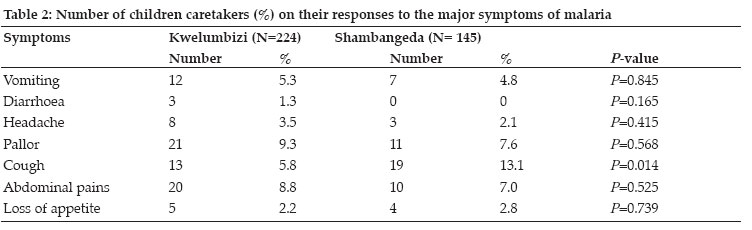
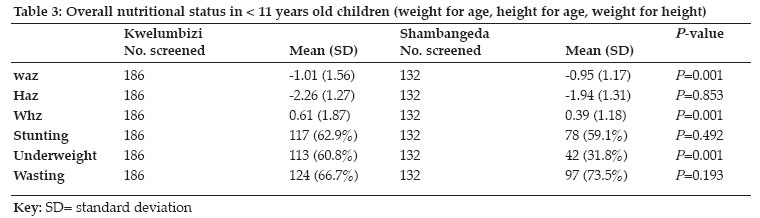
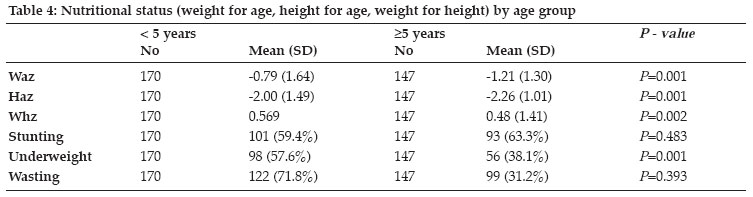
Tanzania Health Research Bulletin, Vol. 8, No. 2, May, 2006 pp. 56-61 Malaria and nutritional status in children living in the East Usambara Mountains, north-eastern Tanzania M.L. KAMUGISHA1*, N. CRAWFORD2, Z. SAVAELI1, H. MSANGENI1, J.J. MASSAGA3, B.P. MMBANDO1 and M.M. LEMNGE1 1Tanga Medical Research Centre, P.O. Box 5004, Tanga, Tanzania * Correspondence : M.L. Kamugisha ; Email : mkamugisha@amani.mimcom.net Code Number: rb06012 Across-sectional survey was conducted in Kwelumbizi and Shambangeda villages, in the East Usambara Mountains, in north-east Tanzania, to determine the prevalence of malaria parasitaemia and nutritional status in children ≤ 11 years old. In addition, knowledge and practice on malaria among the households were determined using questionnaires and focus group discussions. The results showed that prevalence of malaria (48.5 - 51.0%) and parasite density levels was similar in both villages. A significantly higher malaria prevalence was observed in children ≥ 5 years old than in the < 5 years old (P=0.01). This correlated with the higher spleen rate in the same age group (P=0.022). However, higher anaemia prevalence (both severe and moderate), lower haemoglobin levels were found in children < 5 years old. There was no variation in most of the clinical history/symptoms among children with malaria in the two villages. However, coughing (P=0.014) was frequently observed among children in Shambangeda. The use of mosquito nets was more common among the residents of Shambangeda than Kwelumbizi (P=0.001). Children ≥ 5 years old were significantly malnourished in all levels of measurement. Wasting was more frequently observed among females in the < 5year old while stunting and underweight were more observed among males in all age groups. Malaria, anaemia and malnutrition are prevalent in the East Usambara Mountains. Efforts to address these conditions are urgently needed. Key words: malaria, anaemia, nutritional status, children, Tanzania Introduction Malaria is a leading cause of morbidity and mortality in sub-Saharan Africa where the transmission rates are highest and where it is considered to be a major impediment to economic development (Sachs & Malaney, 2002). It is estimated that between 100 and 300 million cases and 1.5-2.7 million deaths occur each year worldwide. Over 90% of the cases occur in sub-Saharan Africa, where the most virulent species, Plasmodium falciparum flourishes (Samba, 2002). In Tanzania, like many other countries in sub-Saharan Africa the pattern of malaria transmission varies markedly from area to area, depending on climate and biogeography. Broad ecological categories have been widely used to describe variations in the observed epidemiological patterns (Clyde, 1967). Such variations in malaria burden are likely to be influenced by several socioeconomic factors. For instance, it has been observed that the behaviour and living conditions of humans may provide an additional risk as a result of an increased exposure to malaria. Moreover, the distribution and ecology of the malaria vectors and the parasites are considered within a context of a climatic and anthropogenic environment, which is in perpetual evolution (Ceccato et al., 2005). Malnutrition and malaria are the most leading cause of child morbidity and mortality globally (Ezzati et al., 2002, Snow et al., 2004). Some studies in Africa have already established some association between malaria and nutritional status among children in developing countries (Jennifer et al., 2003; Alice et al., 2004). For instance, about half of the over more than 10 million deaths that occur annually in underfives in developing countries have been attributed directly or indirectly to malnutrition (Black et al., 2003). In malaria holoendemic areas of coastal Tanzania, a negative effect on malaria infection and nutritional status on children < 5 years old has been reported by Shiff et al. (1996). However, little information is available on the nutritional status among children in areas of moderate malaria transmission, such as the highlands of north-eastern Tanzania. Since 1970s, malaria has been a growing public health problem in the East Usambara Mountains in northeast Tanzania, an area previously considered to be malaria free (Matola et al., 1987). As a result of the growing incidence of malaria in the area, it is important to identify various determinant factors in addition to changes in the environment, community awareness and their accessibility to proper healthcare services. This study was carried out to determine the prevalence of malaria parasitaemia and nutritional status among children living in two adjacent villages in the East Usambara Mountains of northeastern Tanzania. Materials and Methods Study area This study was carried out in Shambangeda and Kwelumbizi villages in the East Usambara Mountains in northeast Tanzania. The area has been previously described by Matola et al (1987) and Ellman et al. (1998). The area lies at >800 m above sea level. It has an annual rainfall of about 1945mm well distributed throughout the year, with peak from March to July. The annual mean temperature is 20.8ºC with a daily maximum of 24.6º C and the minimum of 16.3ºC. The villages of Kwelumbizi and Shambangeda were selected for this study. Kwelumbizi village is located between latitude 4°58'37’ S and longitude 38°39'20’ E and lies at 896.655m above sea level. Shambangeda village is located between latitudes 5°03'29”S, and longitude 38°38'18”E) and lies at 926.795m. The two villages were 21km apart. Malariometric surveys Community-based cross sectional malariometric surveys were conducted in the two villages during August 2004 and involved children aged ≤ 11 years. A physician performed a complete physical examination to each study participant. Children were clinically examined for malaria and spleen sizes and graded according to Hackett's score. Axillary's temperature was measured using a digital thermometer (± 0.1°C percent error). A fever was recorded where the temperature was ≥ 37.5°C. Blood samples were obtained through finger prick method for thick and thin smears. The blood smears were prepared and stained using 10% Giemsa and examined under microscope for presence of malaria parasites. Parasite density was enumerated per 200 leukocytes. A negative slide was delineated as those with no asexual parasites seen after scanning 200 microscopic fields under oil immersion under x100 objective. Those having sexual parasites present were counted against 500 leukocytes. The mean parasite density was log transformed to normalize the data. Haemoglobin (Hb) concentration was determined using a Haemocue machine. Questionnaires were administered to obtain specific demographic data (name, age, sex, village and sub-village) and mosquito control measures practiced within the household. Focus group discussions were also conducted in each village and involved a group of 12 women (with children under 11 years of age). Information regarding health problems and causes of malaria, and health seeking behaviour in the villages was sought. Children diagnosed with clinical malaria and other diseases were advised to seek appropriate treatment from the nearest healthcare facility. Anthropometrics surveys The anthropometrics variables used in this study were age, weight and height. Standard technique and equipment were employed (Gibson, 1990). Weight of a child was measured and recorded to the nearest 100g using Salter scale (Model 235 6S, England) with a capacity of measuring up to 25kg. The scale was adjusted to read zero before starting the measurements. Height was measured using length board. The measurement was recorded while the subject was standing without shoes on a horizontal flat plate attached to the base of the length board with his/her heels together. Data analysis Data from each survey were entered into a database created in Epi Info 2002. Data was then transferred to STATA statistical package version 5 and SPSS 11.5 for Windows to determine statistical relationships between villages. Chi-square tests were used to examine the variation in prevalence of malaria and anaemia between both communities. T-tests were used to examine continuous data, parasite density, spleen rate and haemoglobin levels based on the intensity and blood concentration, respectively for each village. Normal Hb concentration levels were classified as greater than or equal to 11g/dL, moderate Hb concentrations were 6-10g/dL. Children found to have Hb concentration level <5g/dL were classified as having severe anaemia (WHO, 2003). For the anthropometrics indices, the z-scores were calculated with reference to National Centre for Health Statistics (NCHS) standards. Classification of nutritional status basing on standard deviations (SDs) was done according to WHO (1995) cut-off points where below or equal (3SD) were classified as severely stunted, underweight or wasted; between (-3SD) and below (-2SD) were classified as moderately stunted, undernutrition or wasted; between (-2SD) and (+2SD) defined as normal nutritional status and above (+2SD) specified as over-nutrition. Results A total of 380 children (aged 0-11 years) were surveyed and clinically examined; 227 (59.7%) were from Kwelumbizi village and 153 (40.3%) were from Shambangeda village. The mean age was 4.9 and 5.1 years in Kwelumbizi and Shambangeda, children < 5years of age was anaemic as compared respectively. Of these, 172 (45.3%) were males and to 43.7 of children ≥ 5 years. The average mean 208 (54.7%) were females. The sex ratio and mean haemoglobin level for both villages was 10.6 g/dl ages between the two villages were not statistically (range= 4.4 - 16g/dl). There was no variation in different (P> 0.05). haemoglobin levels between the two villages Plasmodium falciparum was the dominant malaria species in the two villages (Kwelumbizi =95.6%; Shambangeda =90.7%). Mixed infection of P. falciparum+P. malariae accounted for 1.6% and 1.3% of all infections in Kwelumbizi and Shambangeda, respectively. Overall, 187 (49.2%) children were found to carry malaria parasites in their blood. The malaria prevalence in Kwelumbizi was 48.5% and in Shambangeda was 51.0%, the difference was not statistically different (P= 0.57). The geometric parasite density index (GMI) in Kwelumbizi and Shambangeda were 1480 (95% CI: 963 - 2122) and 1097 (95% CI: 735 - 1720), respectively (Table 1). In the two villages, a total of 197 (56.9%) children were found to be anaemic (Hb < 11g/dl). The overall prevalence for severe anaemia (Hb < 5g/dl) was 9.0%, and moderate (Hb: 6-10g/dl) was 35.3%. In Shambangeda, 85 (55.6%) of the children were anaemic and none had severe anaemia. In Kwelumbizi, 112 (58.03%) were anaemic, 2 (1.04%) had severe anaemia and 110 (57.0%) had moderate anaemia. Significantly a high proportion (69.8%) of children < 5years of age was anaemic as compared to 43.7 of children ≥ 5 years. The average mean haemoglobin level for both villages was 10.6 g/dl (range= 4.4 - 16g/dl). There was no variation in haemoglobin levels between the two villages (Kwelumbizi = 10.44g/dl and Shambangeda = 10.76g/dl). The mean Hb level of children ≥ 5 years was 11.58 g/dl significantly higher than the 10.04 g/dl found in under five children (P=0.001). From the results of community interview, all (145) caretakers in Shambangeda reported that mosquitoes were a major public health problem in their area. However, only 113 (50.4%) of the respondents in Kwelumbizi (P=0.001) admitted that mosquitoes were a major problem. More households in Shambangeda were using mosquito nets compared to Kwelumbizi (P= 0.003). According to the children caretakers, a total of 52 (14.0%) of the children had a history of fever within two days before the interview. However, only 22 (5.9%) of the children were identified to have a fever when examined (mean temperature ≥ 37.5oC). Eleven (3.0%) children complained of headaches, 1 (0.3%) convulsions, 19 (5.1%) vomiting, 3 (0.8%) diarrhoea, 32 (8.6%) cough, 30 (8.1%) abdominal pain and 9 (2.4%) loss of appetite. There was no significant difference on the clinical history reported between the two villages. However, more children (13.1%) had cough in Shambangeda than in Kwelumbizi (5.75%) (P = 0.014) (Table 2). Anthropometrics analysis showed that on average, a child in the two villages was slightly malnourished compared to the normal population. Village comparison of weight for age and weight for height in Kwelumbizi were -1.01 and 0.61, respectively showing children were significantly malnourished compared to children in Shambangeda with -0.95 and 0.39 mean measurements (P=0.001 and 0.001, respectively). Children in Kwelumbizi also maintained lower height-for-age standards compared to children in Shambangeda, however, the difference was not significant (P> 0.05). Children ≥ 5 years old were significantly malnourished in all levels of measurement, and they were significantly under-weight in Kwelumbizi than in Shambangeda. No significant differences in nourishment were seen in the sex distribution. Wasting was more frequently observed among females in the <5year olds. However, stunting and underweight were more observed among males in all age groups. Overall, the stunting and wasting levels in the two villages were similar (P= 0.492, P=0.193). However, a larger proportion of underweight children were observed in Kwelumbizi (60.8%) than in Shambangeda (31.8%) (P=0.001) (Table 3). Stunting levels were similar in both < 5 and ≥ 5 years age groups (P=0.483). Similarly, wasting levels did not vary between the two age groups (P=0.393). However, a larger proportion of < 5 year old children were underweight that the ≥ 5 years olds (P=0.001). (Table 4) Discussion Findings of our study have shown that P. falciparum is the main malaria species in the area, more so in Kwelumbiza than Shambandenga. Several other studies in the country have shown a similar picture (see Mboera, 2000). The relatively higher (4.7%) of P. malariae found in Shambandega is interesting. Such a higher proportion of the parasite is rare in many areas of the country and the reasons could not be established. The prevalence of malaria infection between the two villages is similar indicating that the two populations are equally exposed to similar risk of transmission. The malaria parasite rate (48 51%) observed in this study was within the range reported in previous studies (Matola et al., 1984), confirming reports of a stable malaria transmission in the Eastern Usambara Mountains. The lower haemoglobin levels and higher proportions of anaemia in children < 5 years was closely associated with higher proportions of under-weight and stunting in children. The lower nutritional measurements found in children ≥ 5 year was mostly likely to have been attributed to recurrent malaria infections in the affected children. Recent studies regarding stunting and its determination of the severity of malaria-related anaemia in African children showed that poor nutritional habits that cause stunting, increase the level that malaria related anaemia (Newton et al., 1997; Menendez et al., 2000). Anaemia remains one of the most intractable public health problems in malaria-endemic countries of Africa (Crawley, 2004). Anaemia characterised by a low level of haemoglobin in the blood among young children, is also a major health problem in Tanzania (TDHS, 2005). The most common cause being nutritional anaemia resulting from inadequate dietary intake of nutrients necessary for the synthesis of haemoglobin, such as iron, folate, vitamin B12, or other nutrients. Anaemia may also results from malaria or parasitic infection. Results from the recent demographic and health survey have shown that seven in ten children in Tanzania have anaemia. Twenty-five percent have mild anaemia, 43% have moderate anaemia and 4% have severe anaemia (TDHS, 2005). Severe anaemia is highest among children 10-11 months. The prevalence of both severe and moderate anaemia in children in the East Usambara Mountains was higher than the national average. The prevalence of malaria and anaemia and parasite density levels varied significantly between the age groups. Age differentiation correlates with the susceptibility, immunity and exposure to parasite. Infants are usually vulnerable to malaria from the age of approximately three months, when immunity acquired from their mother is wearing off. Due to lower immunity, the < 5years children are likely to have more severe infections accounting for groups with higher parasite densities, lower haemoglobin levels, and larger percentage of anaemia. Children over five have higher prevalence of malaria, which accounts for higher levels of exposure to parasite. Nutritional levels in both villages were slightly lower than the average in a normal population, where implications of socio-economic status can serve as explanations for lower overall health status. Verhoef et al. (2002) showed that stunting may determine the severity of malaria-associated anaemia in African children. In conclusion, malaria, anaemia, and malnutrition are prevalent in the East Usambara Mountains, with little variation between adjacent villages. Efforts to address these health problems are urgently needed. Acknowledgements We wish to thank particularly the people of Kwelumbizi and Shambangeda for their cooperation. We are very grateful to Aza Kimambo, Beatrice Semng'ido and the late Donald Mwanjeluka for their excellent field and technical assistance. We thank Ms. Neema Barua, Ms. Latifa Lugogola and Mr. Benson Swai for data entry. Lastly, we would like to extend special appreciation to Dr. Mwele Malecela for facilitating the study. This study received financial assistance from NIMR-IMHOTEP Student Exchange Programme. References
Copyright 2006 - Health User's Trust Fund (HRUTF) The following images related to this document are available:Photo images[rb06012t2.jpg] [rb06012t3.jpg] [rb06012t4.jpg] [rb06012t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}