 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
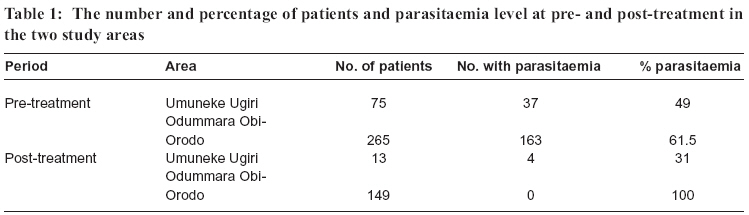
Tanzania Health Research Bulletin, Vol. 8, No. 3, 2006 pp. 183-185 SHORT COMMUNICATION The use of herbs in malaria treatment in parts of Imo State, Nigeria C.N. UKAGA1,* B.E.B. NWOKE 1, P.I.K. ONYEKA1, J.C. ANOSIKE1, O.S. UDUJIH2, O.G. UDUJIH1, R.C. OBILOR1 and M.I. NWACHUKWU2 1Department of Animal and Environmental Biology, Imo State University Owerri, Nigeria 2Department of Microbiology, Imo State University Owerri, Nigeria * Correspondence: Chinyere Ukaga; E-mail:chinyukaga@yahoo.com Code Number: rb06034 Abstract: Persistence of malaria symptoms after treatment with over the counter available antimalarial drugs has resulted in a gradual loss of faith in orthodox drugs. There is thus an increased tendency towards the use of herbs in the treatment of malaria in Imo State, Nigeria. In this study we report activities of two herbalists in the treatment of malaria as well as the effectiveness of the herbal treatment. The study covered two areas namely, Umuneke Ugiri in Isiala Mbano Local Government Area (LGA) and Odummara Obi-Orodo in Mbaitoli LGA of Imo State, Nigeria. A participant–observation technique was used. Finger prick blood samples were collected from patients who visited the herbalists complaining of malaria, and blood smears were stained with Field’s B stain. Blood smears were taken again one-week post – treatment. A total of 75 patients from Umuneke Ugiri and 265 patients from Odumara Obi-Orodo were involved in the study. All the 75 patients (100%) from Umuneke Ugiri and 163 (61.51%) patients from Odummara Obi-Orodo were positive for malaria parasites. Only 13 (17.3%) patients from Umuneke Ugiri and 149 (56.23%) from Odummara Obi-Orodo returned for the post–treatment blood parasite analysis. From Umuneke Ugiri 4 (31%) were still positive for malaria parasite while 9 (69%) were negative. All 149 patients from Odummara Obi-Orodo were negative. This indicates that the herbal treatment was effective. However, there is need for further studies into the efficacy of herbal concoctions, their effective life span, as well as possible toxic effects. Key words: herbal medicines, malaria, treatment, Nigeria Malaria is one of the most important killer diseases in Africa causing more than 1 million deaths every year. In Nigeria, the infection rate has been described as holoendemic (Salako et al., 1994) with more than 75% of children aged 2-9 years infected. In Owerri the capital City of Imo State, a malaria prevalence of 62% was reported in 2005 with 99.7% of the encountered Plasmodium species being Plasmodium falciparium (Ekechukwu, 2005). Malaria is becoming more difficult to manage particularly in areas of multi-drug resistance. It is such a common ailment in Nigeria that most doctors no matter the complaint, first treat for malaria. Moreover, most Nigerians presumably, “know” how to treat themselves for malaria and advices are freely offered for every new method thought to be effective. The uneducated “chemist” or sale persons in drug stores easily prescribe as well as administer drugs to clients who come with complaints of malaria symptoms. Thus self-treatment, incomplete therapy as well as under dosage may have contributed to the development of resistance by the parasite. Many available drugs are no longer able to arrest the ailment. Some must be combined to be effective. Many people have thus sought for relief in the use of herbs and roots. There is increasingly more and more data on herbs, roots, barks, leaves and fruits of various plants believed to be of medicinal value in the treatment of malaria. Many drugs currently in the market for treatment of malaria were developed from herbs. A list of these medicinal plants is available (Oliver-Bever, 1986; Sofoworo, 1993). This present study was aimed at assessing the effectiveness of herbal treatment on the malaria parasite in order to advise the government appropriately. Two villages namely, Umuneke Ugiri in Isiala Mbano Local Government Area (LGA) and Odummara Obi-Orodo in Mbaitoli LGA of Imo State, Nigeria were involved in this study. A herbalist from each village was persuaded after being given enough monetary incentives to be understudied for a period of two weeks. A participant observation technique was used in this study. The herbs and roots used by herbalists were picked with the detailed instructions of the herbalists in the early hours of the mornings and late in the evenings. The preparation of the decoctions was strictly after the herbalist’s directions and under his direct supervision. The dosage was also strictly followed. Finger prick blood samples were taken from volunteer patients pre- and post- treatment. The blood samples were prepared as thick and thin smears, which were stained with Field’s stain B. The herbal plants used by the herbalist from Umuneke Ugiri were identified as’Uvaria chemae locally known as “mmimi – ohia” (used as leaves), Strophantus hispidus locally known as “osisi kaguru” and”Acioa barteria locally known as “ogbodo” (used as roots). The roots and leaves were first washed thoroughly, and then cut into tiny pieces. These were soaked in water for about 2 hours to bring out the active ingredients, and then heated for about 2 minutes. Care was taken not to expose the mixture to too much heat, as heat would destroy the active ingredients. The herbs were then allowed to steep in the water for about 3 minutes after which the resulting concoction was ready for use. A glass (200ml) of the concoction was to be taken twice daily for three days. The herbal plants used by the herbalist from Odummara Obi-Orodo were identified as leaves of Citrus sinensis (sweet orange), Magnifera indica (mango), Carica papaya (paw-paw), Vernonia amygdaline (bitter leaf), Psidum guajava (guava), Ocimum gratissimum (sweet basil), Cymbopogon citrates (lemon grass), Azadirachta indica (neem) and seeds of Citrus aurantifolia (lime). The leaves of guava (P. guajava), paw-paw (C. papaya) lemon grass (C. citratus), neem (A. indica) were all washed thoroughly and boiled together without cutting them into tiny pieces, until there was a colour change. The liquid (decoction) was strained into bottles ready for use. This concoction is called “agbo iba” in the local language. A full glass (200ml) of the decoction was taken 3 times daily for 3 days. When the malaria fever appeared severe, with the patient very weak, the roots of A. barteria and M. lucida were boiled together with the above concoction (to increase the patient’s blood level – according to the herbalist). The dosage remained the same. In cases of very high fever, dried fallen leaves of paw-paw (C. papaya) were put in cold water, and the patient asked to take a cold bath with the water. This is in addition to the oral therapy. Different roots were mixed with leaves in the preparation of a decoction in relation to the symptoms presented by the patients. In mild malaria, leaves of V. amygdalina (bitter leaf) and O. gratissimum (sweet basil) taken in a handful were macerated in 350ml of water, and the liquid strained ready to use. A glass (200ml) of the stained liquid was taken twice daily for 2-3 days. A total of 75 persons volunteered to have their blood taken from Umuneke Ugiri and 265 from Odummara Obi-Orodo. An infection rate of 49.3% (37/75) was noted amongst the volunteers from Umuneke Ugiri, while 61.5% infection rate was recorded for volunteers from Odummara Obi- Orodo (Table 1). Only 13 persons returned for a post– treatment blood assignment from Umuneke Ugiri, while 149 persons from Odummara Obi-Orodo came back for post-treatment blood sampling. There was a 100% clearance of malaria parasites in the blood of the 149 persons from Odummara Obi-Orodo while 4 persons (31%) from Umuneke Ugiri still had malaria parasites (Table 1). The herbalist from Odumara Obi-Orodo appeared to have more therapies for the different forms of malaria, depending on the presentation by the patient unlike that of Umuneke Ugiri. This may explain why the curative rate of the former was higher. The findings of this study are in line with that of Ekanem (1978), who used the same decoction from the leaves of guava (P. guajava), paw-paw (C. papaya) lemon grass (C. citratus) and neem tree (A. indica) on chloroquine sensitive strains of Plasmodium berghei in mice. Okpanyi & Ezeukwu (1981) furthered this finding in showing that the extract from the leaves and bark of the above plants had some antipyretic effects. One of the major approaches to the discovery as well as development of new drugs from plants is to study the plants used locally for the treatment of particular ailments. Most of the drugs used for malaria treatment are synthetic derivation of plant products. A good example is quinine, which is derived from the bark of cinchona tree. Likewise, Artemisinin, extracted from Artemisia annua, is very potent against malaria parasites. There is need for a more extensive research on the use of herbs in malaria therapy. Many people due to economic restrains are resorting more to the readily available, inexpensive method of malaria therapy. There is need to determine the active ingredient in these herbs, and subsequently determine the correct dosage. The herbalists are becoming important members of the community; therefore, they can no longer be ignored. The government should acknowledge the contribution of herbalists to the health sector and organize workshops and seminars for exchange of ideas. The government must devise a means of monitoring the activities of the herbalists; encourage cultivation, conservation and preservation of plants especially medicinal plants. There should be a checklist of medicinal plants in Nigeria and in Africa as a whole. This will help to form a database for medicinal plant research as well as constitute a conservation of the culture of herbalism. References
Copyright 2006 - Health User's Trust Fund (HRUTF) The following images related to this document are available:Photo images[rb06034t1.jpg] |
| |||||||||

{kind=link}